
US health chief says opioid overdose deaths beginning to level off

The number of U.S. drug overdose deaths has begun to level off after years of relentless increases driven by the opioid epidemic, health secretary Alex Azar said Tuesday, cautioning it’s too soon to declare victory. “We are so far from the end of the epidemic, but we are perhaps, at the end of the beginning,” Azar said at a health care event sponsored by the Milken Institute think tank. Confronting the opioid epidemic has been the rare issue uniting Republicans and Democrats in a politically divided nation. A bill providing major funding for treatment was passed under former President Barack Obama. More money followed earlier this year under President Donald Trump. And tomorrow Trump is expected to sign bipartisan legislation passed this month that increases access to treatment, among other steps. More than 70,000 people died of drug overdoses last year, according to preliminary numbers released by the Centers for Disease Control and Prevention this summer— a 10 percent increase from 2016. Health and Human Services — the department Azar heads — is playing a central role in the government’s response. In his speech Azar suggested that multi-pronged efforts to bring the epidemic under control are paying off. He ticked off statistics showing an increase in treatment with medications such as buprenorphine and naltrexone. There’s solid evidence backing medication-assisted treatment, when used alongside counseling and ongoing support. He also noted much broader access to the overdose-reversing drug naloxone, and a documented decline in the number of people misusing prescription opioids as doctors take greater care in prescribing. Azar said that toward the end of last year and through the beginning of this year, the number of deaths “has begun to plateau.” Azar was not indicating that deaths are going down, but noting that they appear to be rising at a slower rate than previously seen. Earlier this month, the CDC released figures — also preliminary — that appear to show a slowdown in overdose deaths in late 2017 and the first three months of this year. From December to March, those figures show that the pace of the increase over the previous 12 months has slowed from 10 percent to 3 percent, according to the preliminary CDC figures. Despite the slowdown, the nation is still in the midst of the deadliest drug overdose epidemic in its history. Opioids were involved in most of the deaths, killing nearly 48,000 people last year. While prescription opioid and heroin deaths appear to be leveling off, deaths involving fentanyl, cocaine and methamphetamines are on the rise. Fentanyl is a synthetic opioid much more powerful than heroin, used as an additive in street drugs. Advocates for people struggling with addiction said they don’t believe the crisis will be quickly or easily resolved. “Even if we are beginning to make a dent in opioid deaths, we still have a really significant problem in this country with addiction, and with the hopelessness and despair so many communities feel,” said Chuck Ingoglia, senior vice president at the National Council for Behavioral Health. In President Barack Obama’s last year in office, his administration secured a commitment to expand treatment and Congress provided $1 billion in grants to states. Trump declared the opioid epidemic a national emergency. Two major funding bills have passed under his watch. While Trump got headlines with his call for using the death penalty against major drug dealers, his administration has built on the treatment approach that Obama favored. The Medicaid expansion in Obama’s Affordable Care Act has also played a critical role, paying for low-income adults to go into treatment. A recent Associated Press analysis showed that states that expanded Medicaid are spending their new opioid grant money from Congress more judiciously, going beyond basics like treatment for people in crisis. Trump tried to repeal the Medicaid expansion, but failed. Advocates for treatment say that they’re pleased that more and more addiction is considered a disease and not a sign of moral weakness. But they say the U.S. has a long way to go build what they call an “infrastructure of care,” a system that incorporates prevention, treatment and recovery. In an interview with The Associated Press this summer, a CDC expert said the overdose death numbers appear to be shifting for the better, but it’s too soon to draw firm conclusions. Month-to-month data show a leveling off in the number of deaths, said Bob Anderson, a senior statistician with the National Center for Health Statistics. However, those numbers are considered preliminary, since death investigations have not been completed in all cases. “It appears at this point that we may have reached a peak and we may start to see a decline,” said Anderson. “This reminds me of what we saw with HIV in the ’90s.” Final numbers for 2018 won’t be available until the end of next year and things could also get worse, not better. Republished with permission from the Associated Press.
Bradley Byrne: SUPPORT in times of crisis

One of the things we pride ourselves on as Alabamians is taking care of each other. Not only should this mean we take care of those we know or our next-door neighbors, it should also mean taking care of all those throughout our region, especially those experiencing hardships. According to the Centers for Disease Control and Prevention, anywhere from 115 to nearly 200 Americans die every day from an opioid overdose. Last year alone, roughly 72,000 people died from this public health crisis. No community or group is exempt from the crisis. This is not a political issue. The opioid epidemic has been going on for far too long, and it is time that something be done about it. It became clear early in the opioid epidemic, as we were just beginning to understand the problem, that treating the opioid crisis would require assistance from every level of government, but also from the private sector. This is more than a single statewide issue, or even a regional issue. The entirety of our country is being affected: every death is another loved one, friend, or neighbor that won’t see their loved ones again. In Congress, we knew we needed to start looking for ways to support those in need in our own backyard, all across the nation. When it comes to a drug crisis like this, prevention comes down to early detection within the community, proper medical treatments, and patient support programs. Last month, the House passed landmark legislation to address the opioid epidemic. Last Wednesday, the Senate passed that bill, known as the SUPPORT for Patients and Communities Act, and it will now be signed into law by President Donald Trump. SUPPORT stands for Substance Use-Disorder Prevention that Promotes Opioid Recovery and Treatment. This multi-pronged solution will be able to better detect, treat, and provide recovery opportunity for those at risk or suffering from opioid abuse or overdose in our communities. Our bipartisan bill will both establish and expand upon early-detection programs to better spot those who may be struggling with opioid addiction. It will also increase health care providers’ ability to treat patients with effective solutions, and it will establish drug management programs for at-risk beneficiaries under Medicaid. This legislation is the most significant congressional action against a single drug crisis in our nation’s history: it is bipartisan, bicameral, and it is a plan that will provide assistance to those who need it most. This legislation comes on top of efforts over the last two years to increase funding for grant programs that help states deal with the opioid crisis. Top-down, government-knows-best solutions rarely work, so I support giving greater resources to allow states and local communities to develop programs that best meet the needs of their residents. Oftentimes we can become wrapped up in our own world of heading to and from work, catching the game, and making sure the kids get to school on time. Rarely do we think of those who may be suffering through the struggles of addiction. But, we are all part of a community, and we cannot fail anyone in our community by not acting. I am proud to say that Congress has done the right thing, and I will continue to support our medical providers, first responders, police officers, and recovery program managers here in Alabama. They need our constant support. I will also keep all those throughout the country who struggle through the awful grips of addiction in my prayers and will continue to look for greater ways we as a community can come together and provide for all our neighbors. • • • Bradley Byrne is a member of U.S. Congress representing Alabama’s 1st Congressional District.
Bradley Byrne: Fighting the opioid epidemic

For too long, a problem of epic proportion has been growing outside of the headlines in the United States: the opioid epidemic. The reality is that we can no longer wait to take action. Drug overdose is now a leading cause of death in the United States. One hundred seventy-five Americans are dying every day from this crisis. From big cities to small towns, the opioid epidemic has hit our communities hard. Unfortunately, Alabama has not been spared. According to the Centers for Disease Control and Prevention (CDC), Alabama ranks highest in the nation as having more opioid prescriptions than people. Alabama also ranks number one as the highest prescribing state in the nation for opioid pain reliever prescriptions. These statistics are incredibly alarming. An opioid is a type of narcotic derived from the opium poppy, which includes drugs such as morphine, codeine, hydrocodone, and oxycodone. While these drugs are often prescribed in response to injuries and body pains, they can be prone to abuse and addiction. The reality is many of the people who become addicted to opioids first start taking the drugs legally after receiving a prescription from a doctor. For example, I have heard testimony from athletes who suffer a sports-related injury, undergo surgery, and then become addicted to opioids during the recovery process. In many cases, this addiction can escalate, driving individuals to street drugs like heroin. Almost all of us have a loved one or know somebody who has been affected by this terrible epidemic. The personal stories are what make this nightmare a harsh reality. Right here in Southwest Alabama, I have heard far too many stories about the dangers of prescription drug abuse. The impacts of this crisis reach far beyond the person suffering from addiction to parents, to children, to brothers and sisters. So many have been hurt. On October 26, 2017, President Donald Trump announced that his administration would declare the opioid crisis a Nationwide Public Health Emergency. On a strongly bipartisan basis alongside President Trump, Congress is also responding. In March, the House voted to set aside $4 million toward combating the opioid crisis in the government funding bill for Fiscal Year 2018. We kept up the momentum last week when the House passed over 25 targeted bills to help prevent and treat opioid addiction and abuse while also ensuring our nation’s drug laws are working to stop the flow of illegal drugs. One such bill that passed the House is the THRIVE Act, which creates a program to provide low-income individuals recovering from opioid and other substance use disorders with a clean, safe, and structured environment following rehabilitation. Additionally, the House passed the STOP Act, which aims to halt opioids like fentanyl from coming into America from other countries through a loophole at the Postal Service. The majority of opioids arrive to America through the mail from other nations, such as China, Mexico and Canada. So, this legislation represents an important step to help solve the problem. It is clear that our work to end the opioid epidemic is far from over. However, I was pleased to see such strong bipartisan support for many opioid bills this week as we work to make a real difference on behalf of the American people. You can learn more about the legislation we are working on at www.opioidcrisis.gop. We cannot and will not sit back and allow the opioid crisis to take the lives of the people we love. We must fight back and ensure Americans get the help they need. I look forward to continuing the work with President Trump to end this epidemic once and for all. • • • Bradley Byrne is a member of U.S. Congress representing Alabama’s 1st Congressional District.
Auburn University research team discovers Zika-transmitting mosquito species in Alabama

Auburn University researchers have discovered the presence of Aedes aegypti — the primary mosquito that transmits Zika virus, yellow fever and other flaviviruses — in Alabama. After a 26-year absence of the mosquito, Sarah Zohdy, Auburn School of Forestry and Wildlife Sciences Assistant Professor of Disease Ecology, and wildlife sciences undergraduate student Victoria Ashby have discovered the species in Mobile. Ae. aegypti was thought to have been eliminated from the state. “Our CDC-funded research has not only allowed for the detection and molecular confirmation of the mosquito in the state, but over the last year we have documented the spread of the mosquito from central Mobile to all of Mobile County,” Zohdy said. The study was conducted from July 2016 to September 2017. Mosquitoes were collected twice a month from the grounds of various tire shops, gas stations, abandoned buildings and open containers quantified to estimate larval abundance. A total of 1,074 mosquitoes were collected, with Ae. aegypti being detected most commonly in the 36606 ZIP code of southwest Mobile, where there were more open containers than any other area in the city. Since 1991, Ae. aegypti was thought to have been displaced in Alabama by another container-breeding mosquito, Ae. albopictus, because Ae. albopictus larvae are better competitors with resource-limited habitats and the males are capable of mating with Ae. aegypti and rendering the females sterile. Despite these advantages, Mobile is the ideal habitat for Ae. aegypti reintroduction or for remnant populations to persist because the city’s maritime traffic and its diverse mix of urban, suburban, rural and industrial environments allow the mosquito to find different habitats where it can either escape from Ae. albopictus or have the competitive upper hand. Aedes aegypti, the primary mosquito that transmits the Zika virus, has been rediscovered in Mobile after a 26-year absence. (CDC) The detection of Ae. aegypti confirms that Alabama residents could be at risk to contract several mosquito-transmitted diseases. “This work demonstrates that citizens of Alabama may be exposed to the mosquito vector of Zika, chikungunya and Dengue fever viruses,” Zohdy said. Zika virus spreads to people primarily through the bite of an infected Aedes species mosquito. Female mosquitoes become infected by ingesting microbes from a person’s blood while biting them and then passing those microbes to the next person’s blood stream. Once infected, the mosquito is then thought to remain infected and able to pass on the virus throughout the remainder of its life, about two to four weeks. During this period they may take three to four blood meals, biting up to four or five people during their lifespan. Ae. aegypti is particularly problematic because it will also bite during the day and is very adaptive to different environments. Specific geographic areas of greatest risk are correlated to the existence of the Aedes species. The Centers for Disease Control and Prevention, or CDC, has developed estimated-range maps using models that predict potential geographic ranges where the Zika-transmitting mosquitoes would likely survive and reproduce based on local and historical records and suitable climate variables. According to the 2017 maps, the Zika-transmitting mosquito species are very likely to exist throughout the southeastern U.S. and as far west as California and as far north as Delaware. Despite Alabama being an ideal habitat for mosquitoes that transmit Zika virus, very little mosquito surveillance data has been collected from around the state. Zohdy said that because of its research efforts and the discovery of Ae. aegypti, her team is now working with the Alabama Department of Public Health. According to the CDC, 449 symptomatic Zika virus disease cases were reported within the U.S. in 2017, with three reported in Alabama and two in Georgia. The majority of cases were instances of travelers contracting the disease from affected areas. Seven cases were acquired through presumed local mosquito-borne transmission — two in Florida and five in Texas. Zohdy’s team is conducting research in all 67 counties in Alabama to determine how widespread Ae. aegypti and Ae. albopictus are across the state. In an effort to crowd-source mosquito surveillance data around the state, Zohdy’s research team has partnered with Prakash Lab at Stanford University to develop and implement an app called “Abuzz,” which will allow Alabama residents to record the sound of a mosquito flying. From this recording, the app can identify the species of mosquito and whether that species could potentially carry a disease by the sound of the buzzing of its wings. Once deployed, the app can empower volunteer “citizen scientists” to participate in mosquito surveillance to help researchers increase the volume and locations of data collection. “Alabama has had little mosquito surveillance in the past, and we hope this app can change that to make it the best-sampled state in the nation,” Zohdy said. Zohdy and her team also surveyed Mobile residents to gain insight about their perceptions of Zika virus and the best ways to target mosquito prevention. Of those responses, 70 percent reported a moderate to very high density of mosquitoes in their home and more than half of those surveyed said they feel concerned to extremely concerned that they or a family member might contract Zika virus. “To help mitigate the threat of the Zika virus it is critical to understand local knowledge and behavioral factors related to exposure to the mosquitoes,” said Wayde Morse, an Auburn School of Forestry and Wildlife Sciences associate professor of human dimensions, who participated in the research efforts. The results of the research were published April 5 in the Journal of Medical Entomology, a scientific journal that historically publishes important information regarding mosquito surveillance. “Having this research published is a good way to reach people who study mosquitoes and other disease vectors,” Zohdy said. Victoria Ashby, a sophomore studying wildlife sciences with a pre-veterinary medicine concentration, has worked with Zohdy’s research team for more than a year and leads fieldwork efforts. “My fieldwork has consisted of biweekly trips down to the Mobile Bay area in order to aspirate for adult mosquitoes and collect larvae using larval dip cups at 25 different sites in 12 ZIP codes,” she said. After graduation, Ashby plans to attend graduate school to continue on the path of disease ecology research and later attend veterinary school. “I have a strong interest in veterinary epidemiology and public health
Pharma Kaleo donates opioid overdose-reversing drugs to Alabama

A major pharmaceutical company previously criticized for inflating prices donated 1,744 doses of an overdose-reversing drug to Alabama’s volunteer rescue squads to combat the opioid crisis, the company announced Wednesday. Kaleo Inc. donated of 872 boxes, which each hold two devices, to carry in state volunteer rescue vehicles, the company announced at a press conference at the Alabama Capitol. The device called Evzio auto-injects the life-saving drug naloxone and contains a voice recording that talks an untrained non-medical professional through administering it. “This is an unbelievable thing happening today, and it’s going to save many lives,” Republican state Sen. Gerald Dial said. Dial said the donation will last Alabama three years. Kaleo Vice President of Corporate Affairs Mark Herzog didn’t commit to extending the grant at the press conference. Dial said he hoped the Alabama legislature would reach a more permanent solution before the drugs run out. Kaleo came under fire for raising the price of the prescription drug from $690 per box in 2014 to $4,500 in 2017. Last month the company said it would sell the drug for $360 to government agencies. Narcan, an alternative device that administers naloxone through nasal spray, costs less than $150 for two doses. There were 756 overdose deaths in Alabama in 2016, the Centers for Disease Control and Prevention reported. The state’s overdose death rate spiked 82 percent over the last decade. CDC said 40 percent of overdoses nationwide are from prescription drugs. Last year, Alabama had the highest national number of opioid prescriptions — more than the state’s total population — according to a report by insurance provider Blue Cross Blue Shield. “Opioid abuse is a tragedy that strikes close to the hearts of communities throughout Alabama, devastating families and destroying lives,” Alabama Attorney General Steve Marshall said in a written statement Wednesday. “One of our most valuable tools is to equip emergency responders with antidote medication that can be a matter of life or death for overdose victims.” In December 2016, the Alabama Department of Public Health issued an order to ensure that naloxone is available to any person at risk of an overdose, even without a prescription for the drug. Alabama Gov. Kay Ivey established a council to combat the opioid crisis in 2017. This year, the Alabama legislature voted into law one of the main recommendations of the council — criminalizing trafficking of fentanyl, one of the most powerful and lethal opioids. The law sets a mandatory minimum sentence for trafficking the drug based on weight. The state will train local volunteer rescue squads to administer naloxone using the donated Evzio device starting Friday. Republished with permission from the Associated Press.
Auburn pharmacy researcher recommends antivirals as key defense this flu season

By: Matt Crouch | Auburn University’s Harrison School of Pharmacy The Centers for Disease Control and Prevention reports the flu is “widespread” across the United States with 48 states reporting widespread activity. With this year’s strain having such an impact, Dr. Marilyn Bulloch, a clinical faculty member in Auburn University’s Harrison School of Pharmacy, suggests the use of antivirals in prevention and treatment. Both the influenza A and influenza B viruses are prominent this year with nearly 15,000 flu-related hospitalizations since October. Vaccines are available through pharmacists and physicians and have shown some resistance to this year’s strain. According to Bulloch, antivirals have shown to be an effective complement to the flu vaccine. “Anyone who is diagnosed with the flu and does not have a reason to not seek therapy can receive antivirals,” said Bulloch. “Studies have shown that they decrease symptoms by several days. This season, the virus has been particularly virulent, and a few days without symptoms such as fever, gastrointestinal upset and muscle aches may help reduce complications of the flu such as hospitalizations.” Current options include Tamiflu (oseltamivir) which is available orally and Relenza (zanamivir), which is an inhalation product that comes as a Diskhaler. For children, Zanamivir is approved for treatment in those over seven and prevention in children over five. Oseltamivir is historically the most common antiviral and can be used for treatment at any age over two-weeks old and for the prevention of influenza in patients over three months of age. There is a one-dose IV product available but it is unknown how many hospitals and urgent care centers have it available. Only Tamiflu is recommended for patients who are hospitalized. There are certain populations that antivirals are strongly recommended this flu season. They include: children over two and adults over 65, those with compromised immune systems, children on long-term aspirin therapy, pregnant women and women who gave birth less than two weeks before influenza diagnosis, American Indians and obese patients with a BMI over 40. Treatment is recommended for patients with certain chronic conditions involving the lung, heart, kidney or liver; those with diabetes, sickle cell, seizures or a history of stroke should also seek antiviral treatment. While it is highly suggested for those populations, anyone with a chronic medical treatment should discuss with their physician the benefit and need for antiviral treatment. “Treatment is most effective when it is started soon after symptom developed, ideally within 48 hours. However, there is some data suggesting patients may still benefit even if treatment is delayed as long as 72 hours after symptom development,” said Bulloch. “Antivirals are recommended for anyone with a severe case of influenza, whose illness is complicated by other issues such as pneumonia, and for those whose influenza does not start to resolve with time.” The good news for those who may come into contact with the flu is that resistance to the medications used to treat it has been almost non-existent this season. While treatments have been effective, prevention is still key and those susceptible to the flu should be prepared. “People who are exposed to those with diagnosed influenza, including household contacts, should strongly consider getting antivirals for the prevention of influenza rather than waiting to become infected,” said Bulloch. For more information on the flu this season, visit www.cdc.gov/flu/. Republished with permission from Auburn University.
State Health Dept. investigates 100 possible flu-related deaths

This season’s aggressive strain of the flu virus has already claimed several lives in Alabama. The Alabama Department of Public Health (ADPH) released updated numbers on Wednesday confirming that influenza has already taken the lives of two children and seven adults, with an additional 98 adult cases under investigation. The flu is a contagious respiratory illness, spread by a virus. The Centers for Disease Control and Prevention (CDC) is reporting this to be the worst influenza season in over a decade. “In severe seasons in the past over 700,000 people have been hospitalized and 56,000 people died from influenza. We may be on track to reach or even exceed those records,” said Anne Schuchat, CDC acting director. Flu season typically runs from October to May, typically peaking in February. Symptoms include sudden onset of fever, headache, extreme fatigue, dry cough, sore throat, runny or stuffy nose, and muscle aches. Children may also have nausea, vomiting and diarrhea. Although most people who get the flu recover in a few days to two weeks, some develop complications like pneumonia that can be life-threatening, the CDC said. Those at highest risk include people 65 and older, people with chronic medical conditions such as asthma, diabetes, or heart disease, pregnant women, and the very young. ADPH said its still not too late to get the flu shot. The chart above indicates ILI activity is still increasing through much of Alabama. [Photo Credit: ADPH]
Southern Research programs aim to shield against pandemic flu dangers
With experts predicting another deadly influenza pandemic in the future, Southern Research scientists are working on several fronts to help limit the death toll from a catastrophic flu outbreak that one day slams the nation. Birmingham-based Southern Research conducts tests on emerging pandemic strains and participates in strategic government vaccine programs focusing on highly pathogenic avian influenza (HPAI) strains that pose potentially grave public health risks. In addition, Southern Research has performed toxicology studies for flu vaccine platforms and provided pre-clinical studies on vaccine candidates, along with clinical trial support for vaccine makers. The nonprofit organization has also researched antiviral treatment approaches that could protect people after infection. “Scientists will tell you it’s not if, it’s when we have a pandemic. That’s the way the flu virus works,” said Landon Westfall, Ph.D., a senior project manager and infectious disease scientist at Southern Research. “It’s like the San Andreas fault – the big one is coming one day. The idea is since we can’t prevent it, we should prepare for it. That’s the goal.” Pandemic influenza strains pose a much greater threat than even the nastiest strains of seasonal flu. The dominant seasonal strain this year, H3N2*, fits that description, causing an above-average rate of hospitalizations and prompting Alabama to declare a public health emergency. The current flu season’s misery is worsened because the available vaccine is only moderately effective. “That’s the challenge with flu. Vaccines don’t always work,” Westfall said. “Most of the time, they protect 55 to 60 percent of the population. That’s kind of the goal of influenza vaccines. But there will always be subsets of the population that won’t be protected.” Elevated dangers Novel avian or swine flu strains, however, have the potential to cause lethal damage on a global scale. Because these dreaded strains are new, very few people have immunity against them, so they can spread widely and rapidly, sickening a large segment of the population, Westfall said. When pandemics emerge, more than half of an affected population can be infected in a single year, while the number of deaths stemming from the flu outbreak can sharply exceed normal levels. The goal is to prevent a global calamity like the 1918 Spanish flu pandemic, which killed more than 50 million people, and outbreaks in 1957 and 1968 that each killed at least 1 million people worldwide. The last pandemic, the 2009 H1N1 swine flu outbreak, killed as many as 575,000 people. More information on pandemics.That’s why the work being conducted by Southern Research and other organizations as part of the U.S. government’s influenza preparedness programs is critically important, Westfall said. For more than a decade, pandemic fears have centered on the highly lethal H5N1 avian influenza, despite the fact that the so-called “bird flu” virus does not infect humans easily. If a mutated form of the H5N1 virus became easily transmissible from person to person while retaining its severe effects, the public health consequences could be very serious, the World Health Organization warns. “For the most part, avian influenza affects birds. When the virus makes a jump from one species to another, say from bird to human, that’s a big thing,” said Westfall, who oversees the influenza virology program for Southern Research’s Drug Development division. “That’s a rapid evolution for a virus that will likely cause major problems. In cases where the avian flu has infected humans, the mortality rate has been around 60 percent.” Southern Research scientists have worked on influenza projects for government agencies including the National Institutes of Health, the National Institute of Allergy and Infectious Diseases, and the Biomedical Advanced Research and Development Authority. The organization has also worked with a number of commercial clients. “We’re recognized as one of the leading supporters for clinical vaccine research, especially for flu,” Westfall said. “That is partly because of our history in the field but also because of our capabilities to test a large volume of samples in a relatively short time.” The next pandemic Although most experts believe another influenza pandemic is inevitable, Westfall said it is impossible to predict when or where it will occur, or how severe its impact will be. It’s almost impossible to predict with certainty the subtype of influenza virus most likely to cause the next worldwide outbreak. While the Centers for Disease Control and Prevention says the risk of H7N9 is currently low because human-to-human transmission is rare, the CDC still rates the strain as having the greatest potential to cause a pandemic.Late in 2017, scientists reported that a new strain of H7N9 avian flu circulating in China showed the ability to transmit easily among animals with highly lethal results, raising alarm about its potential to trigger a global human pandemic. Westfall said the evolving nature of influenza viruses presents tough challenges to the research community. “Flu is like a malleable pathogen that can change from week to week, from month to month, and from region to region,” he said. “Every person who gets infected with the flu basically creates a small change in that virus that’s then passed on to multiple people. Flu constantly changes that way.” *In the designation of influenza subtypes, the H refers to hemagglutinin, a protein found on the surface of flu viruses, while the N refers to viral neuraminidase, another protein present on the surface of the virus. This story originally appeared on the Southern Research website. Republished with permission from the Alabama NewsCenter.
Kay Ivey declares State of Emergency due to widespread flu outbreak
The past month has seen an explosion of influenza (flu) cases across Alabama leading Gov. Kay Ivey to declare a State Public Health Emergency on Thursday. According to the Alabama Department of Public Health (ADPH) Alabama is experiencing widespread flu activity, and hospitals are at or over normal patient capacity due in large part to the number of patients presenting with seasonal influenza-like symptoms. Emergency departments and outpatient clinics are also seeing very high volumes of patients.At this time, this is not a pandemic flu situation, but a major seasonal flu situation. According to the governor’s proclamation, healthcare facilities in the state are overwhelmed by the number of patients with the flu and are taxed to such an extent that care of patients may now no longer be provided in the traditional, normal, and customary manner nor is the utilization of traditional, normal, and customary standards of care possible. The emergency declaration allows those facilities to implement “alternative standards of care” plans. ADPH says alternative standards of care allow medical personnel to both streamline and simplify the support process to preserve lives. The proclamation also states the State of Emergency is to remain in effect until it is rescinded by the governor. Ivey’s declaration follows the Centers for Disease Control and Prevention (CDC) saying the 2018 flu season is expected to be one of the worst in recent years. Widespread cases have been reported in 46 states, including Alabama. According to the CDC, the flu has already resulted in the deaths of over 100 individuals, at least 13 of which were children, since it began in October. To avoid getting and spreading the flu, the ADPH urges the general public to follow “Do 10 – Fight the Flu” actions: Get vaccinated Wash your hands Cover your coughs and sneezes Stay home with fever Stockpile supplies Clean and disinfect Know your office emergency plan Learn home care Call your doctor if symptoms get worse Stay informed Flu can cause mild to severe illness, and at times can lead to death. The flu is different from a cold. The flu usually comes on suddenly. People who have the flu often feel some or all of these symptoms: Fever or feeling feverish/chills Cough Sore throat Runny or stuffy nose Muscle or body aches Headaches Fatigue (tiredness) Some people may have vomiting and diarrhea, although this is more common in children than adults. If you are able to contact your doctor within 48 hours of onset of symptoms, you can potentially be administered an antiviral drug which will reduce the severity of symptoms in addition to the length of the illness.
EPA chemical review would exclude millions of tons of toxins
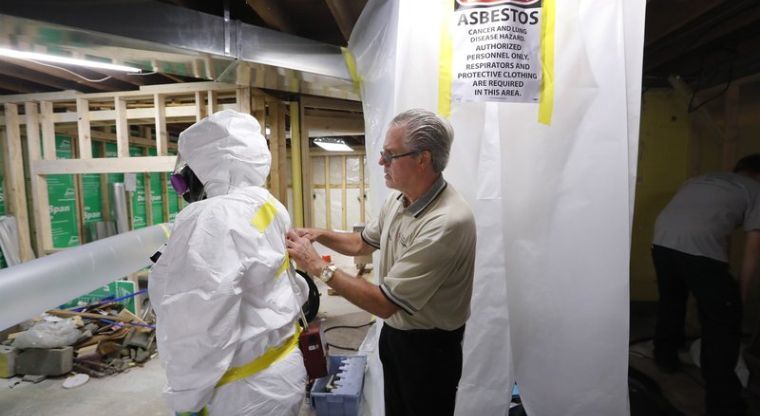
Spurred by the chemical industry, President Donald Trump‘s administration is retreating from a congressionally mandated review of some of the most dangerous chemicals in public use: millions of tons of asbestos, flame retardants and other toxins in homes, offices and industrial plants across the United States. Instead of following President Barack Obama‘s proposal to look at chemicals already in widespread use that result in some of the most common exposures, the new administration wants to limit the review to products still being manufactured and entering the marketplace. For asbestos, that means gauging the risks from just a few hundred tons of the material imported annually while excluding almost all of the estimated 8.9 million tons (8.1 million metric tons) of asbestos-containing products that the U.S. Geological Survey said entered the marketplace between 1970 and 2016. Lawmakers say the review was intended to be the first step toward enacting new regulations needed to protect the public. But critics – including health workers, consumer advocates, members of Congress and environmental groups – contend ignoring products already in use undermines that goal. The administration’s stance is the latest example of Trump siding with industry. In this case, firefighters and construction workers say the move jeopardizes their health. Both groups risk harm from asbestos because of its historical popularity in construction materials ranging from roofing and flooring tiles to insulation used in tens of millions of homes. Most of the insulation came from a mine in a Montana town that’s been declared a U.S. Environmental Protection Agency Superfund site and where hundreds of people have died from asbestos exposure. “Hundreds of thousands of firefighters are going to be affected by this. It is by far the biggest hazard we have out there,” said Patrick Morrison, assistant general president for health and safety at the International Association of Fire Fighters. “My God, these are not just firefighters at risk. There are people that live in these structures and don’t know the danger of asbestos.” Asbestos fibers can become deadly when disturbed in a fire or during remodeling, lodging in the lungs and causing problems including mesothelioma, a form of cancer. The material’s dangers have long been recognized. But a 1989 attempt to ban most asbestos products was overturned by a federal court, and it remains in widespread use. The National Institute for Occupational Safety and Health analyzed cancer-related deaths among 30,000 firefighters from Chicago, Philadelphia and San Francisco. The 2015 study concluded firefighters contract mesothelioma at twice the rate of other U.S. residents. Firefighters also face exposure to flame retardants included in the EPA’s review that are used in furniture and other products. “I believe the chemical industry is killing firefighters,” said Tony Stefani, a former San Francisco fireman who retired in 2003 after 28 years when diagnosed with cancer he believes resulted from exposure to chemicals in the pending review. Stefani said he was one of five in his station to contract cancer in a short period. Three later died, while Stefani had a kidney removed and endured a year of treatment before being declared cancer-free. “When I entered the department in the early 70s, our biggest fear was dying in the line of duty or succumbing to a heart attack,” he said. “Those were the biggest killers, not cancer. But we work in a hazardous-materials situation every time we have a fire now.” Mesothelioma caused or contributed to more than 45,000 deaths nationwide between 1999 and 2015, according to a Centers for Disease Control and Prevention study in March. The number of people dying annually from the disease increased about 5 percent during that time. Congress ordered the EPA review last year to gauge risks of asbestos and nine other highly toxic substances and find better ways to manage them for public safety. In one of its last acts under Obama, the EPA said in January it would judge the chemicals “in a comprehensive way” based on their “known, intended and reasonably foreseen uses.” Under Trump, the agency has aligned with the chemical industry, which sought to narrow the review’s scope. The EPA now says it will focus only on toxins still being manufactured and entering commerce. It won’t consider whether new handling and disposal rules are needed for “legacy,” or previously existing, materials. “EPA considers that such purposes generally fall outside of the circumstances Congress intended EPA to consider,” said EPA spokeswoman Enesta Jones, adding the agency lacks authority to regulate noncommercial uses of the chemicals. One of the law’s co-authors, New Mexico Democratic Sen. Tom Udall, disputes that Congress wanted to limit the review. “It doesn’t matter whether the dangerous substance is no longer being manufactured; if people are still being exposed, then there is still a risk,” Udall told The Associated Press. “Ignoring these circumstances would openly violate the letter and the underlying purpose of the law.” Rep. Frank Pallone of New York, ranking Democrat on the House Energy and Commerce Committee, said the EPA was deferring to the chemical industry’s wishes at the expense of public health. Democrats and public health advocates have criticized EPA Administrator Scott Pruitt for hiring two people – Nancy Beck, the agency’s deputy assistant administrator for chemical safety, and Liz Bowman, its associate administrator for public affairs – who formerly worked for the American Chemistry Council, the industry’s lobbying arm. The council pushed back against the Obama administration’s interpretation of the law, urging the EPA’s new leadership to narrow its review. The Trump administration did that in June. “Did we get everything we wanted? No. But we certainly agree the (Trump) administration put forth a reasonable final rule,” said council vice president Michael Walls. Broadening the review, he added, would send the EPA “down a rabbit hole chasing after illusory risks.” The politically influential National Association of Homebuilders, which represents the residential construction industry, fears broadly interpreting the new law would lead to burdensome regulations that are unnecessary because it says asbestos disposal rules already are adequate. Many of those regulations are based
New Alabama mothers encouraged to complete PRAMS survey

Why are some babies born healthy while others are not? That’s a question the Alabama Department of Public Health (ADPH) and the Centers for Disease Control and Prevention (CDC) is hoping to answer. In a joint research project — Pregnancy Risk Assessment Monitoring System (PRAMS) — the ADPH and CDC are asking recent mothers from across the Yellowhammer State for information about things they experienced before, during, and shortly after pregnancy in an effort to improve the health of mothers and infants by reducing adverse outcomes. Alabama is currently one of 47 states participating in PRAMS. As part of the program, mothers with reported births from across the state are randomly selected to answer the PRAMS survey. “If you receive a survey booklet, please complete it,” Alabama PRAMS Data Manager Victoria Brady said. “The information collected is used in developing health care programs and policies, and the results help doctors and nurses improve health care while making better use of health resources.” The types of questions asked are as follows: Attitudes and feelings about the most recent pregnancy Content and source of prenatal care Mother’s alcohol and tobacco use Any physical abuse before and during pregnancy Infant health care Contraceptive use Health care coverage Mother’s socioeconomic situation Postpartum depression Knowledge of pregnancy-related health issues such as nutrition, the benefits of folic acid, infant safe sleep practices, oral health during pregnancy, and the risks of STDs and HIV Answers will be used for research purposes only and grouped with those of other women. Surveys take about 20 minutes to complete, are available in English and Spanish, and can be mailed back postage-free or completed over the telephone. Mothers may not want to answer a particular question, and that is okay. There is no penalty for not answering all questions. Mothers who complete a survey may choose from among three complimentary items— disposable diapers, an insulated cooler, or a manicure set—that are mailed to them in appreciation for their participation. “Every pregnancy is different, as is every birth,” Brady continued. “Your experience may have a profound effect in bringing about a successful pregnancy and delivery for another mom or even for yourself with a subsequent pregnancy. You can play an active role in improving the health and well-being of Alabama women and babies.”
Bill Miller: The critical ingredient to the success of vaccination programs

Only a few weeks into a new administration and with it comes unwelcome medical news. The age-old debate about the safety and appropriateness of vaccination has been renewed and a vocal stage has been delivered to a small group of anti-vaccination zealots. Reports have circulated that Robert F. Kennedy, Jr, a highly visible critic of vaccination, has been invited to chair a commission on vaccination safety by the new administration. If it comes to pass, one result can be accurately predicted. It will become a confused platform of ideological rhetoric that will diminish trust in those scientific bodies charged with making sound judgments for the public welfare. This inevitable outcome is particularly unfortunate since there has never been any advance in medical history that has had a more positive impact on our lives than vaccination. Humanity has been in eternal conflict with infectious disease throughout history. Perhaps no disease better illustrates the vast range of impacts of epidemic disease than smallpox.In 18th Century Europe, at least 400,000 people died annually from smallpox. One-third of the survivors went blind. Mortality rates were as high as 60% in some communities. Infant mortality was even more frightening, approaching 80%. The ultimate success of smallpox vaccination is credited to Sir Edward Jenner in England. In 1796, he successfully introduced the technique of cowpox vaccination demonstrating its subsequent protective effect against smallpox. Today, due to the effectiveness of worldwide smallpox vaccination programs, that disease has been effectively eradicated from the planet. However, this is not the case for other consequential infectious diseases. Two years ago, a whooping cough epidemic swept through California where vaccination rates are steadily lagging. Contrary to any ordinary expectation, it is often the most affluent parents who are shunning immunization. Some of these anti-vaccine proponents are highly educated people being misled by social media. The trend appears to have originated with a fraudulent report in a British medical journal linking vaccination with autism. This report was subsequently revealed to have been based on fraudulent research and was retracted by that scientific journal. Similar rumors that vaccine stabilizers, such as thimerosol, contribute to autism have also been refuted. Nonetheless, damage has been done by ill-informed repetition. There is no doubt that those parents that refuse to vaccinate their children are well meaning. However, their actions are ill advised on two levels. The first is that refusing to appropriately vaccinate themselves or their child exposes both of them to the risks of deadly infections that can be entirely avoided. Yet, although vaccination is safe and highly effective it does have its limits. This links to the other critical factor that makes universal vaccination so crucial. No vaccination ever devised provides 100% protection and some individuals in any population cannot be vaccinated. This includes very young infants whose immune systems are not yet mature enough for vaccination and members of our community that are immunosuppressed due to diseases that weaken their immune system from a variety of illnesses including cancer. Their protection is through our actions. When there are high levels of vaccination within any community, the infectious agent is unable to find enough hosts to reproduce and sustain itself within that population. This level of community-wide protection is termed herd immunity. It is our joint responsibility, all of us together, to be part of the process of achieving this level of immunity both in our own interests and for the protection of the other members of our community. The next outbreak of a preventable infectious disease with its incumbent tragedies is always lurking. A political committee to examine the evidence based on ideological biases is not needed. Instead, our policies should rely on the expertise of already existing scientific organizations such as the Global Advisory Committee on Vaccine Safety (GACVS), an independent expert clinical and scientific advisory body, as well as our own Centers for Disease Control and the National Institutes of Health. The critical ingredient to the success of vaccination programs is education. Therefore, there needs to be a concerted program to recover our eroded memories of the consequences of now distant epidemic diseases that have been conquered or reduced through vaccination. The success of vaccination programs depends on being familiar with the bitter lessons of our continuous struggle with epidemic disease. Such an educational process must be ever ongoing. ••• Dr. Bill Miller has been a physician in academic and private practice for over 30 years. He is the author of The Microcosm Within: Evolution and Extinction in the Hologenome. He currently serves as a scientific advisor to OmniBiome Therapeutics, a pioneering company in discovering and developing solutions to problems in human fertility and health through management of the human microbiome. For more information, www.themicrocosmwithin.com.

