
Kay Ivey awards grants to strengthen fight against illegal drugs

Gov. Kay Ivey has strengthened the state’s arsenal in the fight against opioids and other illegal or abused drugs by issuing $386,207 in grants to the Alabama Department of Forensic Sciences. Ivey awarded grants of $260,207 and $126,000 that will enable the department to purchase two state-of-the-art substance analyzers capable of rapidly analyzing and identifying prescription and illegal drugs, including opioids. The analyzers are also expected to help reduce a backlog of drug cases. “Evidence provided by the Alabama Department of Forensic Sciences is often the difference between whether a suspect is convicted or set free,” Ivey said. “These new tools will greatly enhance the ability of technicians to accurately examine drug evidence and provide that information to law enforcement agencies and prosecutors.” The analyzers can identify solid and liquid substances to determine the presence and type of drug. Average screening time for each sample is expected to take about two minutes, according to the department. The Department of Forensic Sciences performs evidence collection and identification for more than 450 law enforcement agencies in Alabama. The Alabama Department of Economic and Community Affairs (ADECA) is administering the grants from funds made available to the state from the U.S. Department of Justice (DOJ). “Gov. Ivey recognizes the tireless work that the Department of Forensic Sciences performs daily to assist our law enforcement agencies and prosecutorial services in doing their jobs effectively and efficiently,” ADECA Director Kenneth Boswell said. “ADECA is pleased to join Gov. Ivey in this partnership to provide this new equipment.”
Alabama gets federal assistance to help take drug dealers, drugs off the streets

In the state’s ongoing fight against the drug epidemic, Gov. Kay Ivey has put federal funds in the hands of law enforcement in hopes of reducing illegal drug use in the state by arresting those who buy or sell illegal drugs or falsely obtain prescription drugs. On Thursday, the Alabama Department of Economic and Community Affairs (ADECA) announces Ivey awarded nearly $1.6 million to the Alabama Law Enforcement Agency (ALEA) and the seven regional drug task force offices under ALEA. The task forces were formed in January 2018 and are made up of officers in local law enforcement agencies. “We must combat illegal and illegally obtained drugs that rob so many people of productive lives and destroy families,” Ivey said. “I am pleased to support this task force, and I am grateful to the men and woman who risk their lives to take drugs off our streets.” In less than a year since its inception, the statewide drug task force has been involved in 889 drug cases and has seized 463 pounds of marijuana, 179 pounds of cocaine and 29.3 pounds of heroin and opioids along with other drugs and 312 firearms. The task force is made up of 93 law enforcement officers representing 46 state, county and municipal law enforcement agencies. ALEA and the seven regional drug task force offices each received $197,500 in grant funding. Each regional office covers eight to 12 counties, although officers have powers in other jurisdictions. Funds will be used to cover overtime and operational expenses and equipment purchases. The ADECA is administering the grants from funds made available to the state from the U.S. Department of Justice (DOJ). “ADECA is proud to be a partner with Gov. Ivey and ALEA in this process that takes drugs and dealers off out streets and makes our communities safer,” ADECA Director Kenneth Boswell said.
Donald Trump says new proposal will lower some US drug prices

Less than two weeks before the midterm elections, President Donald Trump on Thursday announced a plan to lower prices for some prescription drugs, saying it would stop unfair practices that force Americans to pay much more than people in other countries for the same medications. “We are taking aim at the global freeloading that forces American consumers to subsidize lower prices in foreign countries through higher prices in our country,” Trump said in a speech at the Department of Health and Human Services. “Same company. Same box. Same pill. Made in the exact same location, and you would go to some countries and it would be 20 percent of the cost of what we pay,” said Trump, who predicted the plan will save Americans billions. “We’re fixing it.” But consumers take note: The plan would not apply to medicines people buy at the pharmacy, just ones administered in a doctor’s office, as are many cancer medications and drugs for immune system problems. Physician-administered drugs can be very expensive, but pharmacy drugs account for the vast majority of what consumers buy. Don’t expect immediate rollbacks. Officials said the complex proposal could take more than a year to put into effect. In another twist, the plan is structured as an experiment through a Medicare innovation center empowered to seek savings by the Affordable Care Act. That’s the law also known as “Obamacare,” which Trump is committed to repealing. Trump has long promised sweeping action to attack drug prices, both as president and when he was running for the White House. He made his latest announcement just ahead of the Nov. 6 elections, with health care high among voters’ concerns. Under the plan, Medicare payment for drugs administered in doctors’ offices would gradually shift to a level based on international prices. Prices in other countries are lower because governments directly negotiate with manufacturers. Drugmakers immediately pushed back, arguing the plan amounts to government price-setting. “The administration is imposing foreign price controls from countries with socialized health care systems that deny their citizens access and discourage innovation,” Stephen Ubl, president of the Pharmaceutical Research and Manufacturers of America, said in a statement. “These proposals are to the detriment of American patients.” Trump is linking the prices Americans complain about to one of his longstanding grievances: foreign countries the president says are taking advantage of U.S. research breakthroughs. Drug pricing expert Peter Bach of Memorial Sloan Kettering’s Center for Health Policy and Outcomes called the plan “a pretty substantive proposal” but one that faces “serious political challenges.” “The rhetoric about finally dealing with foreign freeloading suggests that we are going to take steps to get other countries to pay their fair share for innovation,” Bach added. But that’s “quite literally the opposite of what is being proposed. What is being proposed is that we freeload off of other countries’ ability to negotiate more effectively.” Democratic leaders on Capitol Hill were dismissive. House Minority Leader Nancy Pelosi of California said if Trump wants to save seniors money he should seek congressional approval for Medicare to negotiate prices for its main prescription drug program, “Part D.” Senate Democratic Leader Chuck Schumer of New York said “it’s hard to take the Trump administration and Republicans seriously about reducing health care costs for seniors two weeks before the election.” The health insurance industry, at odds with drugmakers over prices, was pleased with the administration’s action. Matt Eyles, president and CEO of America’s Health Insurance Plans, said: “Drug prices are out of control, and we commend the Administration for its continued commitment to reduce drug prices.” As an experiment, the proposal would apply to half the country. Officials said they’re seeking input on how to select the areas that will take part in the new pricing system. HHS Secretary Alex Azar said politics would have nothing to do with it. In advance of Trump’s speech, HHS released a report that found U.S. prices for the top drugs administered in doctors’ offices are nearly twice as high as in foreign countries. The list includes many cancer drugs. Medicare pays directly for them under its “Part B” coverage for outpatient care. Physician-administered drugs cost Medicare $27 billion in 2016. HHS says the plan would save Medicare $17.2 billion over five years. Beneficiaries would save an estimated $3.4 billion through lower cost-sharing. The plan could meet resistance not only from drugmakers but from doctors, now paid a percentage of the cost of the medications they administer. However, HHS officials said the plan is designed so it would not cut into doctors’ reimbursements. Azar said more plans are being developed on drug costs. “This is not the end of the road, the end of the journey,” he said. “There is more coming.” Trump has harshly criticized the pharmaceutical industry, once asserting that the companies were “getting away with murder.” But it’s largely been business as usual for drugmakers even as Trump has predicted “massive” voluntary price cuts. A recent Associated Press analysis of prices for brand-name drugs found far more increases than cuts in the first seven months of this year. The analysis found 96 price hikes for every price cut. The number of increases slowed somewhat and they were not quite as steep as in past years, the AP found. The Trump administration proposal is open for public comment for 60 days. Republished with permission from the Associated Press.
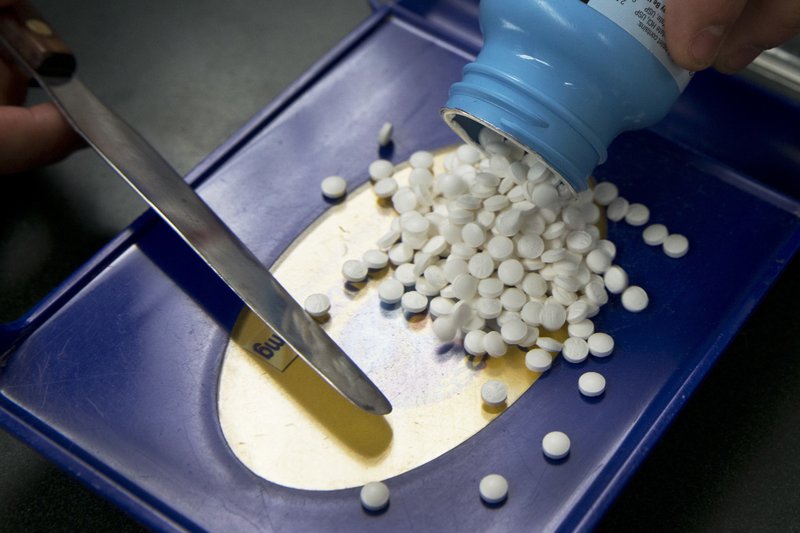
Alabamians encouraged to participate in Prescription Drug Take-Back Day

Do you have unused prescription drugs collecting dust in your medicine cabinet? Well it’s time to clean them out this Saturday. Saturday marks the 16th annual DEA National Prescription Drug Take-Back Day where at approximately 50 collection sites across the state, Alabamians can safely toss their unwanted, unused prescription medications. Sponsored by the U.S. Drug Enforcement Administration (DEA), the program was created to combat the abuse or misuse of potentially dangerous medicines that have expired or are no longer needed for those whom these controlled substances were prescribed. From 10 a.m. to 2 p.m., law enforcement officers will be present at sites across the state to receive unused prescription drugs for safe and proper disposal. Alabama Attorney General Steve Marshall is encouraging Alabamians to participate. “Prescription Drug Take-Back is a valuable public service that protects our children, our homes and our environment,” said Marshall. “As a long-time prosecutor, I have too often witnessed the tragic results caused by the availability of dangerous controlled substances. When prescription drugs are left in our homes, children and teenagers may be poisoned or fall prey to drug abuse and addiction. Your old medications can be a lure to criminals looking for drugs to use or sell.” He continued, “On Saturday, October 27, please take the opportunity to remove these hazards by bringing prescription drugs that are out-of-date or no longer needed to collection sites for their safe and proper disposal.” History of the Take-back event in Alabama Since the first Take-Back event in Alabama, in September of 2010, the program continues to increase in the amount of drugs collected. Throughout all of Alabama’s previous DEA Prescription Drug Take-Back events, a total of about 66,805 pounds of unwanted, unused or expired drugs have been removed and disposed of safely. Deliveries of drugs to DEA Prescription Drug Take-Back Day events are confidential, with no personal information collected and no questions asked. Participants are encouraged to remove labels or black-out information beforehand. A listing of sites may be found through a search at www.DEATakeBack.com. If you do not find your area listed on the DEA website, please check with your local law enforcement officials to see if they may be participating in a Take-Back event.
US health chief says opioid overdose deaths beginning to level off

The number of U.S. drug overdose deaths has begun to level off after years of relentless increases driven by the opioid epidemic, health secretary Alex Azar said Tuesday, cautioning it’s too soon to declare victory. “We are so far from the end of the epidemic, but we are perhaps, at the end of the beginning,” Azar said at a health care event sponsored by the Milken Institute think tank. Confronting the opioid epidemic has been the rare issue uniting Republicans and Democrats in a politically divided nation. A bill providing major funding for treatment was passed under former President Barack Obama. More money followed earlier this year under President Donald Trump. And tomorrow Trump is expected to sign bipartisan legislation passed this month that increases access to treatment, among other steps. More than 70,000 people died of drug overdoses last year, according to preliminary numbers released by the Centers for Disease Control and Prevention this summer— a 10 percent increase from 2016. Health and Human Services — the department Azar heads — is playing a central role in the government’s response. In his speech Azar suggested that multi-pronged efforts to bring the epidemic under control are paying off. He ticked off statistics showing an increase in treatment with medications such as buprenorphine and naltrexone. There’s solid evidence backing medication-assisted treatment, when used alongside counseling and ongoing support. He also noted much broader access to the overdose-reversing drug naloxone, and a documented decline in the number of people misusing prescription opioids as doctors take greater care in prescribing. Azar said that toward the end of last year and through the beginning of this year, the number of deaths “has begun to plateau.” Azar was not indicating that deaths are going down, but noting that they appear to be rising at a slower rate than previously seen. Earlier this month, the CDC released figures — also preliminary — that appear to show a slowdown in overdose deaths in late 2017 and the first three months of this year. From December to March, those figures show that the pace of the increase over the previous 12 months has slowed from 10 percent to 3 percent, according to the preliminary CDC figures. Despite the slowdown, the nation is still in the midst of the deadliest drug overdose epidemic in its history. Opioids were involved in most of the deaths, killing nearly 48,000 people last year. While prescription opioid and heroin deaths appear to be leveling off, deaths involving fentanyl, cocaine and methamphetamines are on the rise. Fentanyl is a synthetic opioid much more powerful than heroin, used as an additive in street drugs. Advocates for people struggling with addiction said they don’t believe the crisis will be quickly or easily resolved. “Even if we are beginning to make a dent in opioid deaths, we still have a really significant problem in this country with addiction, and with the hopelessness and despair so many communities feel,” said Chuck Ingoglia, senior vice president at the National Council for Behavioral Health. In President Barack Obama’s last year in office, his administration secured a commitment to expand treatment and Congress provided $1 billion in grants to states. Trump declared the opioid epidemic a national emergency. Two major funding bills have passed under his watch. While Trump got headlines with his call for using the death penalty against major drug dealers, his administration has built on the treatment approach that Obama favored. The Medicaid expansion in Obama’s Affordable Care Act has also played a critical role, paying for low-income adults to go into treatment. A recent Associated Press analysis showed that states that expanded Medicaid are spending their new opioid grant money from Congress more judiciously, going beyond basics like treatment for people in crisis. Trump tried to repeal the Medicaid expansion, but failed. Advocates for treatment say that they’re pleased that more and more addiction is considered a disease and not a sign of moral weakness. But they say the U.S. has a long way to go build what they call an “infrastructure of care,” a system that incorporates prevention, treatment and recovery. In an interview with The Associated Press this summer, a CDC expert said the overdose death numbers appear to be shifting for the better, but it’s too soon to draw firm conclusions. Month-to-month data show a leveling off in the number of deaths, said Bob Anderson, a senior statistician with the National Center for Health Statistics. However, those numbers are considered preliminary, since death investigations have not been completed in all cases. “It appears at this point that we may have reached a peak and we may start to see a decline,” said Anderson. “This reminds me of what we saw with HIV in the ’90s.” Final numbers for 2018 won’t be available until the end of next year and things could also get worse, not better. Republished with permission from the Associated Press.
Doug Jones’ bill penalizes fentanyl exporters, calls out China
A bipartisan bill aimed at combatting the nation’s ongoing opioid epidemic proposes new penalties on foreign countries that turn a blind eye to drug kingpins who export deadly fentanyl to the United States. Sponsored by Alabama U.S. Sen. Doug Jones and Pennsylvania U.S. Sen. Pat Toomey, the Blocking Deadly Fentanyl Imports Act would make American foreign aid contingent upon a recipient country cooperating with U.S. drug enforcement efforts relating to fentanyl. Under this measure, a fentanyl-producing nation, such as China, would lose access to the Export-Import Bank and be ineligible for other U.S. taxpayer-subsidized aid if it fails to cooperate with the U.S. on narcotics control. “Like many places across the country, Alabama is in the midst of a substance abuse and overdose crisis, in part because of dangerous synthetic drugs like fentanyl,” said Jones. “Fentanyl not only harms those who use it, but it also poses a serious threat to our first responders should they be exposed. This legislation is another smart step to stop illicit fentanyl from being transported across our borders and into our communities.” Fentanyl has caused fatal overdoses across the United States. Sometimes added to heroin or cocaine without the user knowing, fentanyl is 50 to 100 times more potent than heroin and morphine, and can kill those who come in contact with even minuscule amounts of it. Many in law enforcement and the health care industry believe it is drug catalyst of the national opioid epidemic. This measure would also require the State Department to identify in its annual report on narcotics trafficking those countries that are major producers of fentanyl. This requirement is already in place for countries that are major sources of heroin, cocaine, and methamphetamine. “The opioid and heroin epidemic has become increasingly lethal in part due to the widespread presence of illicit fentanyl,” said the bill’s co-sponsor Toomey. “Since fentanyl can be fifty times as potent as heroin, just a tiny amount of this dangerous substance can kill a person, including first responders who may be inadvertently exposed to the drug when responding to an overdose victim or a crime scene. For the sake of our communities and the safety of law enforcement, countries like China must stop illicitly exporting fentanyl and improve their drug enforcement efforts now.” Calling out China’s role in illicit fentanyl exports With deaths from illicit fentanyl sourced from China continuing to climb at dramatic rates, it is clear more needs to be done to stem the flow of this deadly substance into our country. In September 2017 and April 2018, the United States indicted six Chinese nationals in connection with fentanyl manufacturing and distribution. All six charged Chinese nationals remain at large. In November 2017, President Donald Trump requested that China schedule fentanyl as a class, which would effectively place all fentanyl analogues under control.[10] In April 2018, Attorney General Jeff Sessions indicated he was seeking “greater cooperation” from China in sharing bank records in order to reduce illicit fentanyl imports. The Blocking Deadly Fentanyl Imports Act would require countries like China that are major sources of fentanyl to comply with international agreements on narcotics control, give regulators authority to ban new illicit dangerous substances in an emergency, prosecute drug makers who produce fentanyl and fentanyl analogues, and regulate the ownership of pill presses, which are used to produce counterfeit narcotics.
Alabama community health centers receive $4M in critical opioid treatment grants

Community health centers across the state are receiving federal grants to support increased treatment and prevention for opioid and substance abuse. Sen. Richard Shelby made the announcement Thursday that 15 centers would receive a total of $4,038,000 in federal grant funding from the U.S. Department of Health and Human Services (HHS). “It is of the utmost importance that we work to fund the fight against the national opioid crisis,” said Shelby. “Nearly every county in Alabama is affected by this growing problem. These HHS grants will allow community health centers across the state to provide treatment to patients with opioid and substance abuse and support addiction prevention programs, helping our communities tackle this widespread epidemic.” These grants will impact community health centers in the following areas of the state: Bayou La Batre, Birmingham, Centreville, Gadsden, Huntsville, Mobile, Montgomery, Parrish, Selma, Scottsboro, Troy, and Tuscaloosa. On September 19, HHS awarded nearly $352 million to 1,232 community health centers across the nation, including the 15 in Alabama, through the Expanding Access to Quality Substance Use Disorder and Mental Health Services (SUD-MH) awards. The SUD-MH awards support health centers in implementing and advancing evidence-based strategies that best meet the substance use disorder and mental health needs of the populations they serve. The following 15 community health centers in Alabama will receive $4,038,000 in grant funding: Bayou La Batre Area Health Development Board, Inc., Bayou La Batre – $285,000 Christ Health Center, Inc., Birmingham – $285,000 Alabama Regional Medical Services, Birmingham – $285,000 Aletheia House, Inc., Birmingham – $201,750 Cahaba Medical Care Foundation, Centreville – $296,000 Quality of Life Services, Inc., Gadsden – $293,000 Central North Alabama Health, Huntsville – $285,000 Health Services, Inc., Montgomery – $285,000 Franklin Primary Health Center, Inc., Mobile – $285,000 Mobile County Health Department, Mobile – $285,000 Capstone Rural Health Center, Parrish – $287,250 Rural Health Medical Program, Inc., Selma – $285,000 Northeast Alabama Health Services, Inc., Scottsboro – $110,000 S.E. Alabama Rural Health Associates, Troy – $285,000 Whatley Health Services, Inc., Tuscaloosa – $285,000
Lawmakers announce opioid overdose devices for high schools statewide

An auto-injection device that helps reverse an overdose from opioids, like heroin and prescription painkillers, is being offered for free to high schools across the state of Alabama. A group of Alabama state senators made the announcement during a press conference Thursday that the manufacturing company Kaleo Inc. is providing the devices that can help prevent someone from dying from an opioid overdose to public and private schools statewide. Each device normally costs $3,000. Schools interested in getting one will be trained by the Alabama Department of Public Health (ADPH) on how to use the device. In May, Kaleo Inc. donated of 872 boxes, which each hold two devices, to carry in state volunteer rescue vehicles. The device called Evzio auto-injects the life-saving drug naloxone and contains a voice recording that talks an untrained non-medical professional through administering it. On Thursday, Dial said the devices have already saved 15 lives in the state of Alabama. Alabama’s struggle with opioids Alabama is at Ground Zero in the opioid overdose crisis — last year the state had the highest national number of opioid prescriptions, more than the state’s total population, according to a report by insurance provider Blue Cross Blue Shield. “Opioid abuse continues to be one of the most critical issues our society faces — over 49,000 Americans died last year from opioid overdoses,” Dial said. “This affects every family in Alabama, and we need law enforcement agencies, schools, churches, and private companies to come together to rid this scourge from our state.”
Bradley Byrne: Fighting the opioid epidemic
For too long, a problem of epic proportion has been growing outside of the headlines in the United States: the opioid epidemic. The reality is that we can no longer wait to take action. Drug overdose is now a leading cause of death in the United States. One hundred seventy-five Americans are dying every day from this crisis. From big cities to small towns, the opioid epidemic has hit our communities hard. Unfortunately, Alabama has not been spared. According to the Centers for Disease Control and Prevention (CDC), Alabama ranks highest in the nation as having more opioid prescriptions than people. Alabama also ranks number one as the highest prescribing state in the nation for opioid pain reliever prescriptions. These statistics are incredibly alarming. An opioid is a type of narcotic derived from the opium poppy, which includes drugs such as morphine, codeine, hydrocodone, and oxycodone. While these drugs are often prescribed in response to injuries and body pains, they can be prone to abuse and addiction. The reality is many of the people who become addicted to opioids first start taking the drugs legally after receiving a prescription from a doctor. For example, I have heard testimony from athletes who suffer a sports-related injury, undergo surgery, and then become addicted to opioids during the recovery process. In many cases, this addiction can escalate, driving individuals to street drugs like heroin. Almost all of us have a loved one or know somebody who has been affected by this terrible epidemic. The personal stories are what make this nightmare a harsh reality. Right here in Southwest Alabama, I have heard far too many stories about the dangers of prescription drug abuse. The impacts of this crisis reach far beyond the person suffering from addiction to parents, to children, to brothers and sisters. So many have been hurt. On October 26, 2017, President Donald Trump announced that his administration would declare the opioid crisis a Nationwide Public Health Emergency. On a strongly bipartisan basis alongside President Trump, Congress is also responding. In March, the House voted to set aside $4 million toward combating the opioid crisis in the government funding bill for Fiscal Year 2018. We kept up the momentum last week when the House passed over 25 targeted bills to help prevent and treat opioid addiction and abuse while also ensuring our nation’s drug laws are working to stop the flow of illegal drugs. One such bill that passed the House is the THRIVE Act, which creates a program to provide low-income individuals recovering from opioid and other substance use disorders with a clean, safe, and structured environment following rehabilitation. Additionally, the House passed the STOP Act, which aims to halt opioids like fentanyl from coming into America from other countries through a loophole at the Postal Service. The majority of opioids arrive to America through the mail from other nations, such as China, Mexico and Canada. So, this legislation represents an important step to help solve the problem. It is clear that our work to end the opioid epidemic is far from over. However, I was pleased to see such strong bipartisan support for many opioid bills this week as we work to make a real difference on behalf of the American people. You can learn more about the legislation we are working on at www.opioidcrisis.gop. We cannot and will not sit back and allow the opioid crisis to take the lives of the people we love. We must fight back and ensure Americans get the help they need. I look forward to continuing the work with President Trump to end this epidemic once and for all. • • • Bradley Byrne is a member of U.S. Congress representing Alabama’s 1st Congressional District.
Martha Roby: Combating the opioid crisis at home and across the country

There are countless important issues currently facing our state and nation. From our ongoing conversations with North Korea to the continuing need for enhanced security at the southern border, there’s no shortage of priorities that warrant discussion. Unfortunately, there is one very serious issue that continues to make headlines: the horrific opioid epidemic that is gripping our state and the entire country. I’m sure most of us know someone whose life has been affected by opioid abuse. Whether it’s prescription pain relievers or synthetic opioids like fentanyl, the crisis has only gotten worse. 64,070 people died from overdoses in our country in 2016, and 756 of those individuals were Alabamians. Now, in 2018, the problem has not improved. Did you know that 115 people in the United States die after overdosing on opioid drugs every single day? Just this year alone, it is estimated that more than 2 million Americans will suffer from opioid addiction. I’m pleased that last October, President Donald Trump declared the opioid crisis a public health emergency. This epidemic has been wreaking havoc on communities and families across our country for far too long. While the statistics are certainly shocking, this is about so much more than numbers. Hundreds of thousands of real American people with lives, careers, and families have lost the battle with opioid drug abuse. That’s why the House has made combating this crisis a top priority over the last several years. You may remember that back in 2016, Congress passed the Comprehensive Addiction and Recovery Act and the 21st Century Cures Act. Earlier this year, we provided $4 billion in government funding specifically to address the opioid crisis. Building upon this work, the House recently passed dozens of meaningful bills to further combat the opioid epidemic, and I’d like to share the four ways we are using this legislation to help fight this serious issue. First, with the recently passed legislation, the House is focusing on treatment and recovery. Our bills improve and expand access to treatment and recovery services, provide incentives for enhanced care, and establish comprehensive opioid recovery centers. Hundreds of thousands of Americans from all walks of life are currently trapped by addiction, and it is imperative that we provide the resources to treat their addiction and help them recover. Second, we’re aiming for prevention. Opioids are an important part of modern day medical care for pain treatment, but they are prescribed entirely too often – and at alarming rates. Our legislation addresses these high prescribing rates while enhancing prescription drug monitoring programs. We have the technology, and it’s past time we used it to more effectively address this crisis. Our legislation also encourages non-addictive opioid alternatives, when practical, to treat pain, and improves the data that allows us to identify and help at-risk patients before the problem becomes dangerously serious. Third, we’re making efforts to better protect communities of all sizes throughout the country by giving law enforcement the tools necessary to remove dangerous drugs. Our bills also enable us to better intercept illicit opioids at international mail facilities and improve access to federal resources for local communities. Last but certainly not least, we’re fighting fentanyl. The legislation we passed in the House allows us to better tackle these ever-changing synthetic drugs, crack down on foreign shipments of illicit drugs, and provide grants for communities to combat fentanyl that is destroying lives as we speak. I am proud of the efforts we’ve made in the House recently to press forward in our fight against this horrible crisis gripping our state and nation, but our work is far from complete. We owe it to the more than 40,000 Americans who die every year – and their families – to push on until strong progress is made. You can read more about our work to combat the opioid epidemic by visiting www.opioidcrisis.gop. ••• Martha Roby represents Alabama’s Second Congressional District. She lives in Montgomery, Alabama, with her husband Riley and their two children.
In taking on high drug prices, Donald Trump faces a complex nemesis
Before taking office, President Donald Trump railed against the pharmaceutical industry and accused it of “getting away with murder.” The populist rhetoric appears to be giving way to a more nuanced strategy focused on making the pharmaceutical market more open and competitive, with the aim of lowering costs for consumers. It’s an approach that could avoid a direct confrontation with the powerful pharmaceutical lobby, but it could also underwhelm Americans seeking relief from escalating prescription costs. On Friday, Trump is scheduled to give his first speech on an overarching plan to lower drug prices. Administration officials previewing the speech Thursday touted it as the most comprehensive plan to tackle prescription drug costs that any president has ever proposed, but offered few specifics. Officials said the plan would increase competition, create incentives for drugmakers to lower initial prices and slash federal rules that make it harder for private insurers to negotiate lower prices. The result would be lower pharmacy costs for patients — a key Trump campaign promise. The plan will not include giving the federal Medicare program power to directly negotiate prices with drugmakers, they noted. Trump campaigned on the idea, which is vigorously opposed by the pharmaceutical industry. Public outrage over drug costs has been growing for years, because Americans are being squeezed in a number of ways: New medicines for cancer and other life-threatening diseases often launch with prices exceeding $100,000 per year. Drugs for common ailments like diabetes and asthma routinely see price hikes around 10 percent annually. Meanwhile some companies have been buying up once-cheap older drugs and hiking prices by 1,000 percent or more. Since entering the White House, Trump has backed away from reforms directly targeting drugmakers and staffed his administration with appointees who have deep ties to the industry, including his health secretary, Alex Azar, a former top executive at Eli Lilly. Still, administration officials ratcheted up the rhetoric ahead of Trump’s speech. Azar promised bold action. FDA Commissioner Scott Gottlieb — another Trump appointee with industry connections — hinted at a plan to “dismantle” the convoluted system of discounts and rebates between drugmakers and health care middlemen. On Thursday, administration officials also vowed to address foreign governments that rely on U.S. medicines but pay drastically lower prices due to government controls. The U.S. accounts for 70 percent of the world’s brand-name drug profits, according to a White House report released earlier this year. Here are some of the drivers of U.S. prescription drug prices, proposals for reducing the costs and what’s at stake: LACK OF REGULATION Drugmakers generally can charge as much as the market will bear because the U.S. government doesn’t regulate medicine prices, unlike most other countries. Medicare is the largest purchaser of prescription drugs in the nation, covering 60 million seniors and Americans with disabilities, but it is barred by law from directly negotiating lower prices with drugmakers. Democrats have long favored giving Medicare that power, but Republicans traditionally oppose the idea. The powerful pharmaceutical lobby has repeatedly fended off proposals that could lower prices, such as Medicare negotiations or importing drugs from countries that regulate pricing. With no direct government price regulation, the primary check on prices comes from buyers in bulk — such as insurance companies and pharmacy benefit managers, which handle prescription coverage for insurers, employers and other big clients. But because there are so many players in the fragmented system, the discounts achieved in the U.S. are generally far more modest than those in other countries. The result is that the U.S. spends more on medicines than any other nation. In 2015, the U.S. spent $1,162 per person on pharmaceuticals, according to the Organization for Economic Cooperation and Development. That compares with $756 for Canada and $497 for the United Kingdom, both of which have government measures to control drug prices. LACK OF TRANSPARENCY The U.S. system for pricing drugs is notoriously complex, so much that the “real” price for most medicines isn’t clear. Critics contend that this lack of transparency limits competition and drives prices higher. Pharmaceutical companies often launch their drugs with high initial prices. But they argue list prices are merely a starting point for negotiations because they give substantial rebates and discounts to pharmacy benefit managers. Those price concessions are almost never disclosed and it’s unclear what portion actually flows back to consumers. FDA Commissioner Scott Gottlieb and others say the lack of transparency in the current system creates perverse incentives in which drugmakers and other health care companies benefit from rising prices — at the expense of patients. Trump officials have suggested requiring Medicare pharmacy benefit managers to share rebate payments with patients. Another proposal would do away with rebates altogether to encourage more upfront discounts in Medicare. But the benefit managers and insurers say that they use rebates to lower health care premiums overall and that doing away with them would drive up costs. PATENTS AND ANTI-COMPETITIVE TACTICS Patents last longer in the U.S. than most countries, typically giving companies a dozen years of competition-free marketing after a drug launches. Most drugmakers increase their prices annually during this monopoly period, and until recently double-digit price hikes were the norm. Drugmakers also have developed a number of techniques to block competitors from launching lower-cost generic drugs. Companies often tweak drug formulations to extend their patents. In other cases, companies directly pay would-be competitors to stay off the market in so-called “pay-to-delay” deals. Gottlieb has promised a crackdown on some of these techniques used to “game the system.” He’s highlighted a practice in which drugmakers use tightly controlled distribution systems to prevent rival manufacturers from purchasing their drug. This effectively blocks the development of generic versions because generic drugmakers must test their products against the original medicine before they can win FDA approval. PUBLIC PERCEPTION A majority of Americans say bringing down prescription drug prices should be a “top priority” for Trump and Congress, according to recent polling by the Kaiser Family Foundation. And experts who study drug pricing say
VA nominee accused of drunken behavior, reckless prescribing

White House doctor Ronny Jackson exhibited a pattern of recklessly prescribing drugs and drunken behavior, including crashing a government vehicle while intoxicated and doling out such a large supply of a prescription opioid that staffers panicked because they thought the drugs were missing, according to accusations compiled by Democratic staff on the committee considering his nomination as Veterans Affairs secretary. The summary was based on conversations with 23 of Jackson’s current and former colleagues at the White House Medical Unit. It is the latest blow to his nomination to lead the government’s second-largest Cabinet agency. In just a matter of days, the allegations have transformed Jackson’s reputation as a celebrated doctor attending the president to an embattled nominee accused of drinking on the job and over-prescribing drugs. He was seen pacing back and forth on the White House grounds Wednesday. And while the White House put on a full-scale defense of Jackson, spokesman Raj Shah said aides are “of course” preparing for the possibility that he might withdraw. “This is, as the president said, Dr. Jackson’s decision,” Shah said on CNN. Jackson huddled late Wednesday evening with top White House press staff. They declined to comment on the situation. A former colleague who spoke to The Associated Press described Jackson as a gregarious, Type A charmer who knew how to position himself for success — attentive to bosses but also causing unnecessary grief and consternation among colleagues. He said Jackson became known as “Candyman” because of the way he handed out drugs. The ex-colleague spoke on condition of anonymity because of fear of retaliation. The “Candyman” nickname was also cited in the summary released by the Democrats. In a section on Jackson’s prescribing practices, the summary said that in one case, missing Percocet tabs threw members of the White House Medical Unit into a panic — but it turned out he had prescribed a “large supply” of the opioid to a White House Military Office staffer. The allegations also referred to multiple incidents of Jackson’s intoxication while on duty, often on overseas trips. On at least one occasion he was nowhere to be found when his medical help was needed because “he was passed out drunk in his hotel room,” according to the summary. At a Secret Service going-away party, the summary says, Jackson got drunk and wrecked a government vehicle. Jackson has denied allegations of bad behavior and told reporters at the White House he was “still moving ahead as planned.” “I never wrecked a car,” he said. “I have no idea where that is coming from.” Reports of overprescribing and alcohol-related behavior problems can jeopardize a doctor’s license. Many state medical boards allow doctors to keep their licenses and return to practice if they complete special treatment programs and submit to random urine screens. The allegations were publicly released on the day that Jackson’s confirmation hearing was to have been held. The hearing was postponed indefinitely while the allegations against him are reviewed. “He treated the people above him very, very well. He treated the people below him very, very poorly,” Sen. Jon Tester, the ranking Democrat on the Senate Veterans Affairs Committee, told the AP. “It’s not surprising the people above him think he was doing a really, really good job.” White House Press Secretary Sarah Huckabee Sanders said Wednesday that Jackson had passed “at least four independent background checks” that found “no areas of concern.” “He has received more vetting than most nominees,” she said. Marc Short, the White House legislative director, could not say he was confident the allegations were false. He was “not familiar” with car wreck episode. But Short also suggested Tester was airing the allegations for political gain. “It’s quite unusual for a United States senator to take allegations that have not been fully investigated, but to flaunt them to the national public to suggest he’s the ‘candyman’ I think is outrageous,” Short said. Tester, speaking on MSNBC, acknowledged that not all the allegations had been verified. “Am I 100% rock solid sure that he did this? No,” Tester said. “But I’ve seen a pattern here that continues on and on and on.” Jackson met late at the Capitol with a key Republican on the Veterans Affairs Committee, Sen. Thom Tillis of North Carolina. They discussed a variety of subjects — “some were the allegations” — as well as Jackson’s credentials for the job. “It was just getting through the facts,” Tillis said. Veterans groups are dismayed over the continuing uncertainty at the VA, already beset by infighting over improvements to veterans care. “The American Legion is very concerned about the current lack of permanent leadership,” said Denise Rohan, national commander of The American Legion, the nation’s largest veterans organization. A watchdog report requested in 2012 and reviewed by the AP found that Jackson and a rival physician exhibited “unprofessional behaviors” as they engaged in a power struggle over the White House medical unit. That report by the Navy’s Medical Inspector General found a lack of trust in the leadership and low morale among staff members, who described the working environment as “being caught between parents going through a bitter divorce.” It included no references to improper prescribing of drugs or the use of alcohol, as alleged in the summary compiled by the Senate Democratic staff members. The White House has released handwritten reports from Trump and former President Barack Obama praising Jackson’s leadership and medical care and recommending him for promotion. Trump’s first VA secretary, David Shulkin, was dismissed after an ethics scandal and mounting rebellion within the agency. But Jackson has faced numerous questions from lawmakers and veterans groups about whether he has the experience to manage the department of 360,000 employees serving 9 million veterans. Republished with permission from the Associated Press.
