
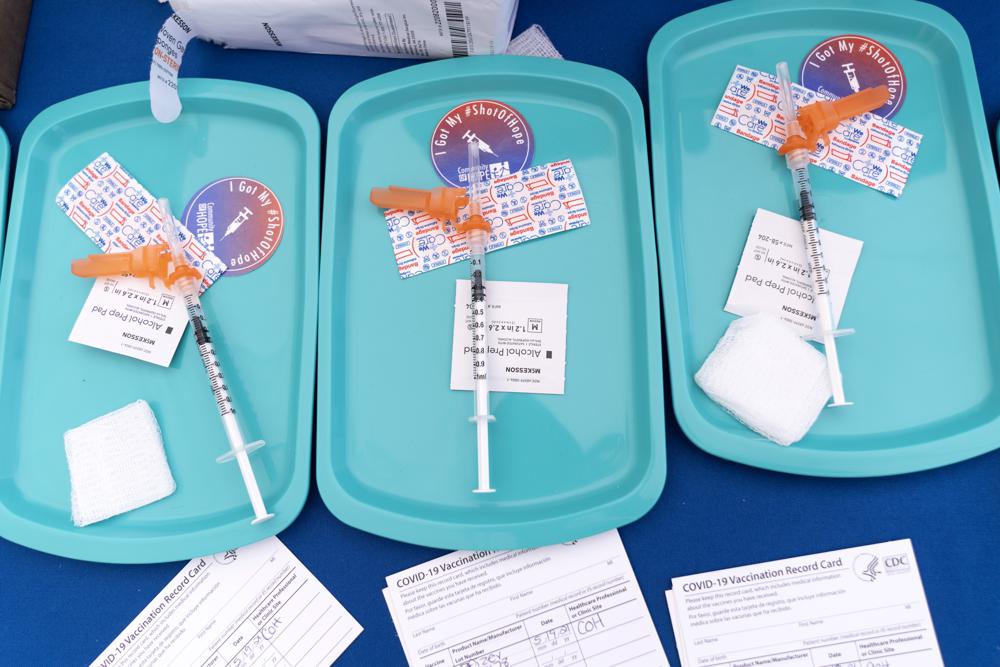
CDC panel recommends Pfizer, Moderna COVID shots over J&J’s

Most Americans should be given the Pfizer or Moderna vaccines instead of the Johnson & Johnson shot that can cause rare but serious blood clots, U.S. health advisers recommended Thursday. The strange clotting problem has caused nine confirmed deaths after J&J vaccinations — while the Pfizer and Moderna vaccines don’t come with that risk and also appear more effective, advisers to the Centers for Disease Control and Prevention said. It’s an unusual move, and the CDC’s director, Dr. Rochelle Walensky, must decide whether to accept the panel’s advice. Until now, the U.S. has treated all three COVID-19 vaccines available to Americans as an equal choice since large studies found they all offered strong protection and early supplies were limited. J&J’s vaccine initially was welcomed as a single-dose option that could be especially important for hard-to-reach groups like homeless people who might not get the needed second dose of the Pfizer or Moderna options. But the CDC’s advisers said Thursday that it was time to recognize a lot has changed since vaccines began rolling out a year ago. More than 200 million Americans are considered fully vaccinated, including about 16 million who got the J&J shot. New data from unprecedented safety tracking of all those vaccinations persuaded the panel that while the blood clots linked to J&J’s vaccine remain very rare, they’re still occurring and not just in younger women as originally thought. In a unanimous vote, the advisers decided the safer Pfizer and Moderna vaccines are preferred. But they said the shot made by J&J’s Janssen division still should be available if someone really wants it — or has a severe allergy to the other options. “I would not recommend the Janssen vaccine to my family members,” but some patients may — and should be able to — choose that shot, said CDC adviser Dr. Beth Bell of the University of Washington. The clotting problems first came up last spring, with the J&J shot in the U.S. and with a similar vaccine made by AstraZeneca that is used in other countries. Eventually, U.S. regulators decided the benefits of J&J’s one-and-done vaccine outweighed what was considered a very rare risk — as long as recipients were warned. European regulators likewise continued to recommend AstraZeneca’s two-dose vaccine although, because early reports were mostly in younger women, some countries issued age restrictions. COVID-19 causes deadly blood clots, too. But the vaccine-linked kind is different, believed to form because of a rogue immune reaction to the J&J and AstraZeneca vaccines because of how they’re made. It forms in unusual places, such as veins that drain blood from the brain, and in patients who also develop abnormally low levels of the platelets that form clots. Symptoms of the unusual clots, dubbed “thrombosis with thrombocytopenia syndrome,” include severe headaches a week or two after the J&J vaccination — not right away — as well as abdominal pain and nausea. While it’s still very rare, the Food and Drug Administration told health care providers this week that more cases have occurred after J&J vaccinations since the spring. They occur most in women ages 30 to 49 — about once for every 100,000 doses administered, the FDA said. Overall, the government has confirmed 54 clot cases— 37 in women and 17 in men, and nine deaths that included two men, the CDC’s Dr. Isaac See said Thursday. He said two additional deaths are suspected. The CDC decides how vaccines should be used in the U.S., and its advisers called the continuing deaths troubling. In comparing the pros and cons of all the vaccines, the panelists agreed that side effects from the Pfizer and Moderna vaccines weren’t as serious — and that supplies now are plentiful. Nor is J&J still considered a one-and-done vaccine, several advisers noted. The single-dose option didn’t prove quite as protective as two doses of the Pfizer and Moderna vaccines. Plus, with extra-contagious virus mutants now spreading, booster doses now are recommended. Several countries, including Canada, already have policies that give preference to the Pfizer and Moderna vaccines. But J&J told the committee its vaccine still offers strong protection and is a critical option, especially in parts of the world without plentiful vaccine supplies or for people who don’t want a two-dose shot. While blood clots are rare, “unfortunately cases of COVID-19 are not,” J&J’s Dr. Penny Heaton said. The U.S. is fortunate in its vaccine availability, and Thursday’s action shouldn’t discourage use of J&J’s vaccine in places around the world where it’s needed, said CDC adviser Dr. Matthew Daley of Kaiser Permanente Colorado. The FDA also warned this week that another dose of the J&J vaccine shouldn’t be given to anyone who developed a clot following either a J&J or AstraZeneca shot. The committee also heard some of the first data on reported side effects of Pfizer vaccinations in younger children. Early last month, the CDC recommended a two-dose series for that age group, and more than 7 million doses have been given so far. But few problems have been reported. Of the 80 reported cases of serious side effects, about 10 involved a form of inflammation that has been seen in male teens and young adults. Republished with the permission of the Associated Press.
FDA OKs mixing COVID vaccines; backs Moderna, J&J boosters

U.S. regulators on Wednesday signed off on extending COVID-19 boosters to Americans who got the Moderna or Johnson & Johnson vaccine and said anyone eligible for an extra dose can get a brand different from the one they received initially. The Food and Drug Administration’s decisions mark a big step toward expanding the U.S. booster campaign, which began with extra doses of the Pfizer vaccine last month. But before more people roll up their sleeves, the Centers for Disease Control and Prevention will consult an expert panel Thursday before finalizing official recommendations for who should get boosters and when. The latest moves would expand by tens of millions the number of Americans eligible for boosters and formally allow “mixing and matching” of shots — making it simpler to get another dose, especially for people who had a side effect from one brand but still want the proven protection of vaccination. Specifically, the FDA authorized a third Moderna shot for seniors and others at high risk from COVID-19 because of their health problems, jobs, or living conditions — six months after their last shot. One big change: Moderna’s booster will be half the dose that’s used for the first two shots, based on company data showing that was plenty to rev up immunity again. For J&J’s single-shot vaccine, the FDA said all U.S. recipients, no matter their age, could get a second dose at least two months following their initial vaccination. The FDA rulings differ because the vaccines are made differently, with different dosing schedules — and the J&J vaccine has consistently shown a lower level of effectiveness than either of the two-shot Moderna and Pfizer vaccines. As for mixing and matching, the FDA said it’s OK to use any brand for the booster regardless of which vaccination people got first. The interchangeability of the shots is expected to speed the booster campaign, particularly in nursing homes and other institutional settings where residents have received different shots over time. FDA’s acting commissioner Dr. Janet Woodcock said the agency wanted to make its booster guidance as flexible as possible, given that many people don’t remember which brand they first received. In other cases, some people may want to try a different vaccine if they previously experienced common side effects like muscle ache or chills. Still, regulators said it’s likely many people will stick with the same vaccine brand. The decision was based on preliminary results from a government study of different booster combinations that showed an extra dose of any type revs up levels of virus-fighting antibodies. That study also showed recipients of the single-dose J&J vaccination had a far bigger response if they got a full-strength Moderna booster or a Pfizer booster rather than a second J&J shot. The study didn’t test the half-dose Moderna booster. Health authorities stress that the priority still is getting first shots to about 65 million eligible Americans who remain unvaccinated. But the booster campaign is meant to shore up protection against the virus amid signs that vaccine effectiveness is waning against mild infections, even though all three brands continue to protect against hospitalization and death. “Today the currently available data suggest waning immunity in some populations of fully vaccinated people,” Woodcock told reporters. “The availability of these authorized boosters is important for continued protection against COVID-19 disease.” The Moderna booster decision essentially matches FDA’s ruling that high-risk groups are eligible for the Pfizer vaccine, which is made with the same technology. FDA recommended that everyone who’d gotten the single-shot J&J vaccine get a booster since it has consistently shown lower protection than its two-shot rivals. And several independent FDA advisers who backed the booster decision suggested J&J’s vaccine should have originally been designed to require two doses. Experts continue to debate the rationale of the booster campaign. Some warn that the U.S. government hasn’t clearly articulated the goals of boosters given that the shots continue to head off the worst effects of COVID-19, and wonder if the aim is to tamp down on virus spread by curbing, at least temporarily, milder infections. FDA’s top vaccine official suggested regulators would move quickly to expand boosters to lower age groups, such as people in their 40s and 50s, if warranted. “We are watching this very closely and will take action as appropriate to make sure that the maximum protection is provided to the population,” said FDA’s Dr. Peter Marks. In August, the Biden administration announced plans for an across-the-board booster campaign aimed at all U.S. adults, but outside experts have repeatedly argued against such a sweeping effort. On Thursday an influential panel convened by the CDC is expected to offer more specifics on who should get boosters and when. Their recommendations are subject to approval by the CDC director. The vast majority of the nearly 190 million Americans who are fully vaccinated against COVID-19 have received the Pfizer or Moderna options, while about 15 million have received the J&J vaccine. Republished with the permission of the Associated Press.
White House details plan to vaccinate 28 million children age 5-11
Children ages 5 to 11 will soon be able to get a COVID-19 shot at their pediatrician’s office, local pharmacy, and potentially even their school, the White House said Wednesday as it detailed plans for the expected authorization of the Pfizer shot for elementary school youngsters in a matter of weeks. Federal regulators will meet over the next two weeks to weigh the safety and effectiveness of giving low-dose shots to the roughly 28 million children in that age group. Within hours of formal approval, which is expected after the Food and Drug Administration signs off and a Centers for Disease Control and Prevention advisory panel meets on Nov. 2-3, millions of doses will begin going out to providers across the country, along with the smaller needles needed for injecting young children. Within days of that, the vaccine will be ready to go into arms on a wide scale. “We’re completing the operational planning to ensure vaccinations for kids ages 5 to 11 are available, easy and convenient,” White House COVID-19 coordinator Jeff Zients said. “We’re going to be ready, pending the FDA and CDC decision.” The Pfizer vaccine requires two doses three weeks apart and a two-week wait for full protection to kick in, meaning the first youngsters in line will be fully covered by Christmas. Some parents can hardly wait. Dr. Sterling Ransone said his rural Deltaville, Virginia, office is already getting calls from people asking for appointments for their children and saying, “I want my shot now.” “Judging by the number of calls, I think we’re going to be slammed for the first several weeks,” said Ransone, president of the American Academy of Family Physicians. Justin Shady, a film and TV writer in Chicago, said his 6-year-old daughter, Grey, got nervous when he told her she would be getting the shots soon. But he is bribing her with a trip to Disney World, and “she’s all in.” The family likes to travel, “we really just want to get back in the swing of seeing the world,” Shady said. As for youngsters under 5, Pfizer and Moderna are studying their vaccines in children down to 6 months old, with results expected later in the year. The Biden administration noted that the expansion of shots to children under 12 will not look like the start of the country’s vaccine rollout ten months ago when limited doses and inadequate capacity meant a painstaking wait for many Americans. The country now has ample supplies of the Pfizer shot to vaccinate the children who will soon be eligible, officials said, and they have been working for months to ensure widespread availability of shots. About 15 million doses will be shipped to providers across the U.S. in the first week after approval, the White House said. More than 25,000 pediatricians and primary care providers have already signed on to dispense the vaccine to elementary school children, the White House said, in addition to the tens of thousands of drugstores that are already administering shots to adults. Hundreds of school- and community-based clinics will also be funded and supported by the Federal Emergency Management Agency to help speed the process. In addition to doctors’ offices, schools are likely to be popular spots for the shots. In Maryland, state officials have offered to help schools set up vaccination clinics. Denver’s public schools plan to hold mass vaccination events for young children, along with smaller clinics offering shots during the school day and in the evenings. Chicago’s public health department is working closely with schools, which have already been hosting vaccination events for students age 12 and older and their families. The White House is also preparing a stepped-up campaign to educate parents and children about the safety of the shots and the ease of getting them. As has been the case for adult vaccinations, the administration believes trusted messengers — educators, doctors, and community leaders — will be vital to encouraging vaccinations. Dr. Lisa Reed, medical director for family medicine at MAHEC, a western North Carolina safety net provider that serves patients from rural Appalachia and more urban communities such as the tourist town of Asheville, said it is going to take effort to get some families on board. Reed said she lives “in a community that has a lot of vaccine hesitancy, unfortunately.” “Some have lower health literacy or belong to ethnic groups that are more hesitant in general” because of a history of mistrust, she said. And Asheville, she said, has a sizeable population of well-educated adults who are longtime vaccine skeptics. While children run a lower risk than older people of getting seriously ill from COVID-19, at least 637 people age 18 or under have died from the virus in the U.S., according to the CDC. Six million U.S. children have been infected, 1 million of them since early September amid the spread of the more contagious delta variant, the American Academy of Pediatrics says. Health officials believe that expanding the vaccine drive will not only curb the alarming number of infections in children but also reduce the spread of the virus to vulnerable adults. It could also help schools stay open, and youngsters get back on track academically, and contribute to the nation’s broader recovery from the pandemic. “COVID has also disrupted our kids’ lives. It’s made school harder, it’s disrupted their ability to see friends and family, it’s made youth sports more challenging,” U.S. Surgeon General Dr. Vivek Murthy told NBC. “Getting our kids vaccinated, we have the prospect of protecting them, but also getting all of those activities back that are so important to our children.” Murthy said the administration, which is imposing vaccine mandates for millions of adults, is leaving it up to state and local officials to decide whether to require schoolchildren to get vaccinated. But he said such measures would be “a reasonable thing to consider.” “It’s also consistent with what we’ve done for other childhood vaccines, like measles, mumps, polio,” he said. The U.S. has
COVID-19 and pregnancy: Women regret not getting the vaccine

Sometimes when she’s feeding her infant daughter, Amanda Harrison is overcome with emotion and has to wipe away tears of gratitude. She is lucky to be here, holding her baby. Harrison was 29 weeks pregnant and unvaccinated when she got sick with COVID-19 in August. Her symptoms were mild at first, but she suddenly felt like she couldn’t breathe. Living in Phenix City, Alabama, she was intubated and flown to a hospital in Birmingham, where doctors delivered baby Lake two months early and put Harrison on life support. Kyndal Nipper, who hails from outside Columbus, Georgia, had only a brief bout with COVID-19 but a more tragic outcome. She was weeks away from giving birth in July when she lost her baby, a boy she and her husband planned to name Jack. Now Harrison and Nipper are sharing their stories in an attempt to persuade pregnant women to get COVID-19 vaccinations to protect themselves and their babies. Their warnings come amid a sharp increase in the number of severely ill pregnant women that led to 22 pregnant women dying from COVID in August, a one-month record. “We made a commitment that we would do anything in our power to educate and advocate for our boy because no other family should have to go through this,” Nipper said of herself and her husband. Harrison said she will “nicely argue to the bitter end” that pregnant women get vaccinated “because it could literally save your life.” Since the pandemic began, health officials have reported more than 125,000 cases and at least 161 deaths of pregnant women from COVID-19 in the U.S., according to the U.S. Centers for Disease Control and Prevention. And over the past several months, hospitals and doctors in virus hot spots have reported a sharp increase in the number of severely ill pregnant women. With just 31% of pregnant women nationwide vaccinated, the CDC issued an urgent advisory on Sept. 29 recommending that they get the shots. The agency cautioned that COVID-19 in pregnancy can cause preterm birth and other adverse outcomes and that stillbirths have been reported. Dr. Akila Subramaniam, an assistant professor in the maternal-fetal medicine division of the University of Alabama at Birmingham, said the hospital saw a marked rise in the number of critically ill pregnant women during July and August. She said a study there found the delta variant of COVID-19 is associated with increased rates of severe disease in pregnant women and increased rates of preterm birth. “Is it because the delta variant is just more infectious or is it because delta is more severe? I don’t think we know the answer to that,” Subramaniam said. When COVID-19 vaccines became available to pregnant women in their states this spring, both Harrison, 36, and Nipper, 29, decided to wait. The shots didn’t have final approval from the Food and Drug Administration and pregnant women weren’t included in studies that led to emergency authorization, so initial guidance stopped short of fully recommending vaccination for them. Pfizer shots received formal approval in August. The women live on opposite sides of the Alabama-Georgia line, an area that was hit hard by the delta variant this summer. While Harrison had to be put on life support, Nipper’s symptoms were more subtle. When she was eight months pregnant, she lost her sense of smell and developed a fever. The symptoms went away quickly, but Jack didn’t seem to be kicking as much as he had been. She tried drinking a caffeinated beverage: Nothing. She headed to the hospital in Columbus, Georgia, for fetal monitoring where medical staff delivered the news: Baby Jack was gone. “He was supposed to come into the world in three weeks or less,” Nipper said. “And for them to tell you there’s no heartbeat and there is no movement …” Nipper’s doctor, Timothy Villegas, said testing showed the placenta itself was infected with the virus and displayed patterns of inflammation similar to the lungs of people who died of COVID-19. The infection likely caused the baby’s death by affecting its ability to get oxygen and nutrients, Villegas said. The doctor said he has since learned of similar cases from other physicians. “We’re at that point where everybody is starting to raise some red flags,” he said. In west Alabama, Dr. Cheree Melton, a family medicine physician who specializes in obstetrics and teaches at the University of Alabama, said she and her colleagues have had about a half-dozen unvaccinated patients infected with COVID-19 lose unborn children to either miscarriages or stillbirth, a problem that worsened with delta’s spread. “It’s absolutely heartbreaking to tell a mom that she will never get to hold her living child,” she said. “We have had to do that very often, more so than I remember doing over the last couple of years.” Melton said she encourages every unvaccinated pregnant woman she treats to get the shots, but that many haven’t. She said rumors and misinformation have been a problem. “I get everything from, ‘Well, somebody told me that it may cause me to be infertile in the future to, ‘It may harm my baby,’” she said. Nipper said she wishes she had asked more questions about the vaccine. “Looking back, I know I did everything that I could have possibly done to give him a healthy life,” she said. “The only thing I didn’t do, and I’ll have to carry with me, is I didn’t get the vaccine.” Now home from the hospital with a healthy baby, Harrison says she feels profound gratitude — tempered with survivor’s guilt. “I cry all the time. Just little things. Feeding her or hugging my 4-year-old. Just the thought of them having to go through life without me and that’s a lot of people’s reality right now,” Harrison said. “It was very scary and it all could have been prevented if I had gotten a vaccination.” Republished with the permission of the Associated Press.
Merck says experimental pill cuts worst effects of COVID-19

Drugmaker Merck said Friday that its experimental COVID-19 pill reduced hospitalizations and deaths by half in people recently infected with the coronavirus and that it would soon ask health officials in the U.S. and around the world to authorize its use. If cleared, the drug would be the first pill shown to treat COVID-19, a potentially major advance in efforts to fight the pandemic. All COVID-19 therapies now authorized in the U.S. require an IV or injection. Merck and its partner Ridgeback Biotherapeutics said early results showed patients who received the drug, called molnupiravir, within five days of COVID-19 symptoms had about half the rate of hospitalization and death as patients who received a dummy pill. The study tracked 775 adults with mild-to-moderate COVID-19 who were considered at higher risk for severe disease due to health problems such as obesity, diabetes, or heart disease. Among patients taking molnupiravir, 7.3% were either hospitalized or died at the end of 30 days, compared with 14.1% of those getting the dummy pill. There were no deaths in the drug group after that time period compared with eight deaths in the placebo group, according to Merck. The results were released by the company and have not been peer-reviewed by outside experts, the usual procedure for vetting new medical research. Merck said it plans to present them at a future medical meeting. An independent group of medical experts monitoring the trial recommended stopping it early because the interim results were so strong. That is typical when early results so clearly show treatment works that there is no need for further testing before applying for authorization. Company executives said they plan to submit the data for review by the Food and Drug Administration in the coming days. Once the submission is complete, the FDA could make a decision within weeks — and, if approved, the drug could be on the market soon after. “It exceeded what I thought the drug might be able to do in this clinical trial,” said Dr. Dean Li, vice president of Merck Research Laboratories. “When you see a 50% reduction in hospitalization or death, that’s a substantial clinical impact.” Side effects were reported by both groups in the Merck trial, but they were slightly more common among the group that received a dummy pill. The company did not specify the problems. Patients take the pill twice a day for five days to complete a course of treatment. Earlier study results showed the drug did not benefit patients who were already hospitalized with severe disease. The U.S. has approved one antiviral drug, remdesivir, specifically for COVID-19, and allowed emergency use of three antibody therapies that help the immune system fight the virus. But all the drugs have to be given by IV or injection at hospitals or medical clinics, and supplies have been stretched by the latest surge of the delta variant. Health experts, including the top U.S. infectious disease expert Dr. Anthony Fauci have long called for a convenient pill that patients could take when COVID-19 symptoms first appear, much the way the standard flu medication Tamiflu helps fight influenza. Such medications are seen as key to controlling future waves of infection and reducing the impact of the pandemic. Merck’s pill works by interfering with the coronavirus’s ability to copy its genetic code and reproduce itself. It has shown similar activity against other viruses. The U.S. government has committed to purchase 1.7 million doses of the drug if it is authorized by the FDA. Merck has said it can produce 10 million doses by the end of the year and has contracts with governments worldwide. The company has not announced prices. Several other companies, including Pfizer and Roche, are studying similar drugs that could report results in the coming weeks and months. Merck had planned to enroll more than 1,500 patients in its late-stage trial before the independent board stopped it early. The results reported Friday included patients enrolled across Latin America, Europe, and Africa. Executives estimated about 10% of patients studied were from the U.S. Republished with the permission of the Associated Press.
U.S. has enough COVID-19 vaccines for boosters, kids’ shots

With more than 40 million doses of coronavirus vaccines available, U.S. health authorities said they’re confident there will be enough for both qualified older Americans seeking booster shots and the young children for whom initial vaccines are expected to be approved in the not-too-distant future. The spike in demand — expected following last week’s federal recommendation on booster shots — would be the first significant jump in months. More than 70 million Americans remain unvaccinated despite the enticement of lottery prizes, free food or gifts, and pleas from exhausted health care workers as the average number of deaths per day climbed to more than 1,900 in recent weeks. Federal and state health authorities said the current supply and steady production of more doses can easily accommodate those seeking boosters or initial vaccination, avoiding a repeat of the frustratingly slow rollout of COVID-19 vaccines across the country early this year. “I hope that we have the level of interest in the booster … that we need more vaccines,” Colorado Gov. Jared Polis said Tuesday. “That’s simply not where we are today. We have plenty of vaccines.” Robust supply in the U.S enabled President Joe Biden this week to promise an additional 500 million of Pfizer’s COVID-19 shots to share with the world, doubling the United States’ global contribution. Aid groups and health organizations have pushed the U.S. and other countries to improve vaccine access in countries where even the most vulnerable people haven’t had a shot. Among the challenges states face is not ordering too many doses and letting them go to waste. Several states with low vaccination rates, including Idaho and Kansas, have reported throwing away thousands of expired doses or are struggling to use vaccines nearing expiration this fall. While most vaccines can stay on the shelf unopened for months, once a vial is opened the clock starts ticking. Vaccines are only usable for six to 12 hours, depending on the manufacturer, according to the U.S. Food and Drug Administration. Moderna vaccines come in vials containing 11 to 15 doses. Pfizer vials contain up to six doses and Johnson & Johnson vials five doses. “We are going to see more doses that go unused over time,” said Wisconsin’s health secretary, Karen Timberlake. “They come in multidose files. They don’t come in nice, tidy individual single-serving packages.” State health officials said they have tried to request only what health care providers and pharmacies expect to need from the federal supply. Those numbers have dwindled since the vaccines became widely available in early spring. But U.S. officials — holding out hope that some of the unvaccinated will change their minds — are trying to keep enough vaccines in stock so all Americans can get them. That balancing act is tricky and can lead to consternation around the globe as the U.S. sits on unused vaccines while many countries in places such as Africa can’t get enough vaccines. “Somebody sitting in a country with few resources to access vaccines, seeing people in the U.S. able to walk into a pharmacy and get that vaccine and choosing not to, I’m sure that’s causing heartache,” said Jen Kates, senior vice president and director of global health and HIV policy for the Kaiser Family Foundation. Dr. Marcus Plescia, chief medical officer of the Association of State and Territorial Health Officials, which represents the public health agencies of all 50 U.S. states, the District of Columbia, and U.S. territories, said officials anticipate that on-hand doses of COVID-19 vaccines and manufacturers’ ability to supply more will meet needs across the country. “I think states have tried to plan as if everybody’s going to be offered a booster,” he said, suggesting they will be overprepared for the more narrow recommendations issued by the FDA and the Centers for Disease Control and Prevention. California, for example, estimated earlier this month that it would need to administer an extra 63 million doses by the end of 2022 — if initial shots for children under 12 were approved and boosters were open to everyone. U.S. health officials late Thursday endorsed booster shots of the Pfizer vaccine for all Americans 65 and older — along with tens of millions of younger people who are at higher risk from the coronavirus because of health conditions or their jobs. California, with nearly 40 million residents, has the lowest transmission rate of any state and nearly 70% of eligible residents are fully vaccinated. That leaves nearly 12 million people not vaccinated or not fully vaccinated. Dr. Mark Ghaly, California’s health secretary, said the state will rely largely on pharmacies and primary care providers to give boosters to seniors while some large counties and health care groups will use mass vaccination sites. In Pennsylvania, more than 67% of residents older than 18 are fully vaccinated. Alison Beam, acting secretary of health, said health authorities now have “two missions”: Continuing to persuade people to get vaccinated and serving those eager to receive a booster or initial shots. “Pennsylvania is going to be prepared,” Beam said. “And we’re going to have the right level of vaccine and vaccinators to be able to meet that demand.” Republished with the permission of the Associated Press.
U.S. regulators give full approval to Pfizer COVID-19 vaccine

The U.S. gave full approval to Pfizer’s COVID-19 vaccine Monday, potentially boosting public confidence in the shots and instantly opening the way for more universities, companies, and local governments to make vaccinations mandatory. The Pentagon promptly announced it will press ahead with plans to force members of the military to get vaccinated amid the battle against the extra-contagious delta variant. The University of Minnesota likewise said it will require its students to get the shot, as did Louisiana’s major public universities, including LSU, though state law there allows broad exemptions. More than 200 million Pfizer doses have been administered in the U.S. under emergency provisions — and hundreds of millions more worldwide — since December. In going a step further and granting full approval, the Food and Drug Administration cited months of real-world evidence that serious side effects are extremely rare. President Joe Biden said that for those who hesitated to get the vaccine until it received what he dubbed the “gold standard” of FDA approval, “the moment you’ve been waiting for is here.” “Please get vaccinated today,” he said. Pfizer CEO Albert Bourla called the FDA’s action “an important milestone that I think will unlock some of the more skeptical minds.” Pfizer said the U.S. is the first country to grant full approval of its vaccine, in a process that required a 360,000-page application and rigorous inspections. Never before has the FDA has so much evidence to judge a shot’s safety. The formula, jointly developed with Germany’s BioNTech, will be marketed under the brand name Comirnaty. Moderna has also applied to the FDA for full approval of its vaccine. Johnson & Johnson, maker of the third option in the U.S., said it hopes to do so later this year. Just over half of the U.S. population is fully vaccinated. Vaccinations in this country bottomed out in July at an average of about a half-million shots per day, down from a peak of 3.4 million a day in mid-April. As the delta variant fills hospital beds, shots are on the rise again, with a million a day given Thursday, Friday, and Saturday. Full approval of Pfizer’s COVID-19 vaccine means it meets the same “very high standards required of all the approved vaccines we rely on every day,” said Dr. Jesse Goodman of Georgetown University, a former FDA vaccine chief. That should help “anyone who still has concerns gain confidence” in the shots. Earlier this month, Defense Secretary Lloyd Austin said he would seek the president’s OK to make the vaccine mandatory by mid-September or once the FDA grants final approval, whichever comes first. On Monday, after the FDA acted, the Pentagon said guidance on vaccinations will be worked out, and a timeline will be provided in the coming days. The approval also opened the way for swift action by colleges to require vaccines and solidified the legal ground for hundreds of universities that have already issued mandates for students and staff. The public university systems in Louisiana and Minnesota had been waiting for FDA action before making vaccinations mandatory. Louisiana has become a COVID-19 hot spot, repeatedly breaking records for the number of people hospitalized with the virus. But certain other states forbid universities to require shots, including Texas and Florida. “Mandating becomes much easier when you have full approval,” said Dr. Carlos del Rio of Emory University. “I think a lot of businesses have been waiting for it.” On the same day the FDA decision came down, New York City announced that all public school teachers and other staffers will have to get vaccinated. The delta variant has sent cases, deaths, and hospitalizations soaring in recent weeks in the U.S., erasing months of progress. Deaths are running at about 1,000 a day on average for the first time since mid-March, and new cases are averaging 147,000 a day, a level last seen at the end of January. Elizabeth Nichols, 18, of Akron, Ohio, said she felt “a rush of relief” after hearing the news of the FDA’s approval. She already was on her way to get her first vaccine shot Monday morning after months of hesitation. “I had an internal battle of whether I should get the shot or not,” Nichols said in an email. “It can be scary subjecting yourself to something that is unapproved.” But she added: “The authorization proves how safe it is.” The FDA, like regulators in Europe and much of the rest of the world, initially allowed emergency use of Pfizer’s vaccine based on a study that tracked 44,000 people 16 and older for at least two months — the time period when serious side effects typically arise. That’s shorter than the six months of safety data normally required for full approval. So Pfizer kept that study going, and the FDA also examined real-world safety evidence. Pfizer’s shot will continue to be dispensed to 12- to 15-year-olds under an emergency use authorization until the company files its application for full approval. Normally, doctors can prescribe FDA-approved products for other reasons than their original use. But FDA’s acting Commissioner Dr. Janet Woodcock strongly warned that the Pfizer vaccine should not be used “off-label” for children under 12 — a warning echoed by the American Academy of Pediatrics. Both Pfizer and Moderna have vaccine studies underway in youngsters, and they are using lower doses than those available for people 12 and older. Pfizer’s Bourla said he expects study results from 5- to 11-year-olds by the end of September, but data for those younger than 5 will take a couple of months. Also, Woodcock said health providers are offering COVID-19 vaccines under agreements with the government that should preclude using Monday’s approval as a pretext for offering booster shots to the general population. Currently, the FDA has authorized third doses of either Pfizer’s or Moderna’s vaccine only for certain people with severely weakened immune systems, such as organ transplant recipients. For everyone else, the Biden administration is planning for boosters starting in the fall. But the
Anthony Fauci hopeful COVID vaccines get full OK by FDA within weeks

The U.S. government’s top infectious disease expert, Dr. Anthony Fauci, said Sunday that he was hopeful the Food and Drug Administration will give full approval to the coronavirus vaccine by month’s end and predicted the potential move will spur a wave of vaccine mandates in the private sector as well as schools and universities. The FDA has only granted emergency-use approval of the Pfizer, Moderna, and Johnson & Johnson vaccines, but the agency is expected to soon give full approval to Pfizer. The Biden administration has stated that the federal government will not mandate vaccinations beyond the federal workforce but is increasingly urging state and local governments as well as businesses to consider such mandates. Fauci, who is President Joe Biden’s chief medical adviser, said “mandates at the local level need to be done” to help curb the spread of the virus. “I hope — I don’t predict — I hope that it will be within the next few weeks. I hope it’s within the month of August,” Fauci said of FDA approval of the vaccine. “If that’s the case, you’re going to see the empowerment of local enterprises, giving mandates that could be colleges, universities, places of business, a whole variety, and I strongly support that. The time has come. … We’ve got to go the extra step to get people vaccinated.” Fauci’s comments come as the Biden administration is weighing what levers it can push to encourage more unvaccinated Americans to get their shots as the delta variant continues to surge through much of the United States. Biden recently approved rules requiring federal workers to provide proof of vaccination or face regular testing, mask mandates, and travel restrictions. Biden is also awaiting a formal recommendation from Defense Secretary Lloyd Austin on potentially requiring U.S. troops to get vaccinated. The administration has become more vocal in its support of vaccine mandates at a moment when high-profile companies have informed employees that coronavirus vaccination requirements are in the works, and some localities have adopted or are contemplating vaccine requirements to dine indoors. United Airlines informed its employees that they will need to be fully vaccinated by Oct. 25 or five weeks after the FDA grants full approval to one of the vaccines — whichever date comes first. Disney and Walmart have announced vaccine mandates for white-collar workers, and Microsoft, Google, and Facebook said they will require proof of vaccination for employees and visitors to their U.S. offices. Tyson Foods has also announced it will require all U.S. employees to get vaccinated by November. There’s also been pushback. The U.S. Supreme Court last week was asked to block a plan by Indiana University to require students and employees to get vaccinated against COVID-19. It’s the first time the high court has been asked to weigh in on a vaccine mandate and comes as some corporations, states, and cities are also contemplating or have adopted vaccine requirements for workers or even to dine indoors. Randi Weingarten, president of the American Federation of Teachers union, said on Sunday that she personally supports a vaccine mandate for educators. “As a matter of personal conscience, I think that we need to be working with our employers — not opposing them on vaccine mandates,” said Weingarten, who estimated about 90% of AFT members are already vaccinated. Dr. Francis Collins, director of the National Institutes of Health, on Sunday all but endorsed vaccine mandates, saying, “I celebrate when I see businesses deciding that they’re going to mandate that for their employees.” “Yes, I think we ought to use every public health tool we can when people are dying,” Collins said. Fauci and Weingarten spoke on NBC’s “Meet the Press,” and Collins appeared on ABC’s “This Week.” Republished with the permission of the Associated Press.
FDA: 38 sick from tainted eggs from Alabama

The government says 38 people in seven states have gotten sick from eggs produced by an Alabama poultry farm. The Food and Drug Administration says the illnesses are linked to salmonella-tainted eggs from Gravel Ridge Farms, which is north of Birmingham in Cullman. The agency issued a recall notice last month, and it provided an update Tuesday. The FDA says 10 people were hospitalized after coming in contact with cage-free eggs from the farm, but no one has died. The government says recalled eggs were sold to several grocery stores in Georgia, Tennessee, and Alabama. Most of the illnesses are in Tennessee, where 23 people have been affected. Alabama has had seven cases and Ohio has four. Single cases have occurred in Colorado, Iowa, Kentucky and Montana. Republished with permission from the Associated Press.
Daniel Sutter: Are we making the opioid problem worse?

Opioid abuse is taking a tremendous toll on America, with 42,000 opioid-related deaths in 2016. The problem involves both prescription opioid-based painkillers and illegal heroin and fentanyl. Might our public policy response be worsening this terrible problem? Economists have analyzed prohibition, both alcohol in the 1920s and illegal drugs more recently. We evaluate prohibition, or any other government policy, by comparing the world with and without the policy in question. This necessarily involves a state of the world which does not exist. We will never see the toll opioids would have taken in 2018 if we had significantly different policies in place. We must construct an alternative. Rules govern the construction of alternatives to produce meaningful comparisons. One key is allowing only the policy to vary, not other factors, so differences can be attributed to alternative policy. For example, prohibition does not automatically stop people from taking a substance. Some potential users will be deterred because of illegality, but others won’t, as we saw with alcohol in the 1920s. Economic analysis distinguishes harm from the substance itself and those due to prohibition. Drug violence, for example, is almost entirely due to prohibition. Dealers’ cash and drugs are vulnerable to theft, and these thefts will not be reported to the police. Dealers will use violence to protect, steal or retrieve drugs and money. Walgreens and CVS do not have gun battles to control the OxyContin market. Prescription painkillers provide a distinctive twist to the opioid crisis. Introduction of opioid painkillers in the 1990s opened new options for millions of American pain sufferers. Prescription drugs occupy a middle ground in prohibition, legal under government-approved conditions and illegal otherwise. Perhaps the major controversy for policy and lawsuits brought by dozens of states and cities against drug companies is the addictiveness of opioid painkillers. Studies in leading medical journals show that perhaps one or two percent of patients using the drugs as prescribed become dependent. Many of the Americans addicted to painkillers obtained them on the black market or through a bogus prescription. In 2010, the Food and Drug Administration reformulated OxyContin to make the pills harder to crush and make into more potent opioids. Other restrictions on prescribing followed, and pill mills have been shut down. Yet the crisis has become much deadlier since 2010, with heroin- and fentanyl-related deaths increasing by factors of five and six respectively, with only a slight decline in prescription-related deaths. (Overdose victims often used more than one narcotic, so deaths are described only as related to a drug.) Heroin, especially when laced with fentanyl, is far deadlier than prescription opioids. It is tragic when people fall into substance abuse, which often happens after traumatic life events. Rehab is often not effective until people decide to change their lives. Unfortunately, public policy may only be able to limit the harm during a dark period in people’s lives, and ensure the availability of help when requested. Forcing people to turn to heroin by restricting access to painkillers increases harm. Restricting access to prescription opioids is costly. Many people can no longer successfully manage their chronic pain, with tragic consequences. In some documented cases, patients have committed suicide after being denied painkillers. Any policy limiting access for people who do not “need” painkillers will deny some patients in pain needed help because pain is subjective; no doctor or nurse can know if it is tolerable. And a strong argument exists that American adults should be able to decide how to treat their pain without the government’s approval. Libertarian psychiatrist Thomas Szasz argued that free people have a right to drugs. The concentration of the opioid deaths in regions with dwindling manufacturing and mining jobs suggests a significant economic element to the crisis. And this, to me, is the crisis’ most disturbing element. America today boasts tremendous prosperity and opportunity. Given the high overall quality of life today, why is the economy seemingly leading so many Americans to addiction? ••• Daniel Sutter is the Charles G. Koch Professor of Economics with the Manuel H. Johnson Center for Political Economy at Troy University and host of Econversations on TrojanVision. The opinions expressed in this column are the author’s and do not necessarily reflect the views of Troy University.
Fate hazy for GOP bill helping dying patients try new drugs

A leading House Democrat announced his opposition Monday to a Republican bill making it easier for some terminally ill patients to try experimental drugs, clouding the measure’s fate. Republicans are hoping for House approval Tuesday, seven months after a similar package cleared the Senate. The “Right to Try” bill gained added momentum after President Donald Trump called for its passage in January’s State of the Union address. Under the bill, if a doctor and drug maker agree to let a patient with life-threatening ailments try an experimental treatment, the federal Food and Drug Administration would no longer need to consent. The FDA would have to be notified of the decision and of any problems that occur. New Jersey Rep. Frank Pallone, top Democrat on the House Energy and Commerce Committee, said the measure is risky, unneeded and “provides false hope to patients.” He also noted that the bill doesn’t require drug makers to provide these treatments to patients, which is often where stumbling blocks can occur. Companies sometimes prefer using what they’ve produced for clinical trials needed for final FDA approval, or worry that a problem could hurt the drug’s marketing prospects. A recent study by the Government Accountability Office, Congress’ investigative agency, found the FDA currently approves 99 percent of such requests, often within hours. The measure strikes a balance between safety and providing “hopeful news for patients desperately seeking the right way to try” experimental treatments, said Energy and Commerce Chairman Greg Walden of Oregon and Michael Burgess of Texas, another top panel Republican. Pallone’s stance is important because GOP leaders want to rush the legislation through the House using a process, normally reserved for uncontroversial measures, that could require a two-thirds majority. If all Republicans vote yes, they’d need the backing of at least 50 Democrats. House Minority Leader Nancy Pelosi, D-Calif., hadn’t taken a public position on the bill by late Monday afternoon. Republicans released the latest version of their proposal Saturday. More than 40 patients’ groups have expressed opposition to the measure, saying it would “likely do more harm than good.” PhRMA, the trade group representing major drug companies, has taken no public stance. Republished with the permission of the Associated Press.
Mo Brooks fights for patients’ ‘Right to Try’
On Thursday, Alabama 5th District U.S. Congressman Mo Brooks delivered a house floor speech requesting a vote on S. 204: the Right to Try Act, which gives terminally ill patients the option to try experimental treatments that have not yet been approved by the Food and Drug Administration (FDA). Often the FDA’s approval of new treatments is a lengthy and complex processes that can takes decades to fully be completed. This bill would allow terminally ill patients to try potentially life-saving experimental treatments and gives patients the right to fight their diseases without having to fight federal bureaucracy. “Patients shouldn’t have to give up their liberty, their freedom, their fight against terminal illness merely because the FDA says so” said Brooks. Brooks was inspired by the story of Steve Mayfield, a beloved football coach at Central High School in Lauderdale County Alabama. Mayfield died in March of 2017 after a long and arduous battle with both Lou Gehrig’s disease (ALS) and the FDA. Like most terminally ill Americans, Mayfield did not have access to investigative treatments due to the FDA’s current policies. “While the Food and Drug Administration grants compassionate use waivers, meant to allow terminal patients access to experimental drugs, only about 1,500 waivers were granted in 2016” said Brooks. “What are other terminally ill Americans to do? Nothing? Just waste away and die without a fight?” Brooks believes the Right to Try Act is the best solution to this problem as it only grants access to treatments that have successfully completed the FDA’s Phase 1 approval requirement. This keeps patients safe from potentially harmful treatment processes while allowing them access to try potentially life changing medical care. “Given the stark contrasts between life and death, between freedom and federal dictates, between hope and hopelessness, the House should take up and pass the Right to Try Act, thereby giving a chance for life to terminally ill patients and their families.” The Senate passed Right to Try legislation last year, and it currently awaits a vote in the House.
